Immature Teratoma and Teratoma Associated with Associated with Malignancies, Clinicopathological and Survival Outcome at AHPGIC
Received Date: September 06, 2021 Accepted Date: October 06, 2021 Published Date: October 08, 2021
doi: 10.17303/jocr.2021.2.104
Citation:Smruti Sudha Pattnaik (2021) Immature Teratoma and Teratoma Associated with Associated with Malignancies, Clinicopathological and Survival Outcome at AHPGIC. JJ Oncol Clin Res 2: 1-19.
Abstract
Aim:To analyse the clinicopathogical features and the survival outcome of the nine cases of teratoma and immature teratoma associated with malignancies and immature teratoma alone.
Material Methods:The Case Included 1. HPS Confirmed Immature teratoma and teratoma with Malignancies After Staging Laparotomy 2. HPS Confirmed Cases of Immature Teratoma Statistical Method of Analysis - Chi square test and Kaplan meyer survival analysis.
Results:The overall survival of immature teratoma is 66.7% with 95% confidence interval (.706, 1.000). The total survival in case of immature teratoma with associated is ther maignancies 66.7% with CI (.300, 1.000). In other hand the total survival in case of immature teratoma with other malignancies is 33.3% with CI (.0673, 1.000). This variability in the two groups of immature teratoma associated with malignancies is probably due two type of asscciated malignancies i.e embryonal and yolk sac and melanoma. The cases teratoma with squamos cell carcinoma all survived. Chi-square test on histology, shows there is no significant difference of survival pattern between different histology types at 5% level of significance. The total survival in case of low grade is 85.7% with CI (.633, 1.000). The total survival in case of high grade is 0.01%; which means there are very low survival in case of high-grade carcinoma. The total survival in case of Conservative surgery is 50% with CI (.225, 1.000); which means there are almost 50% survival in case of Conservative surgery. There is no death event happened in case of Radical surgery so survival cannot be estimated in such case. Thus, there is no significant difference of survival pattern between different treatment types at 5% level of significance (p= 0.2).
Introduction
An immature teratoma is a teratoma that contains anaplastic immature elements, and is often synonymous with malignant teratoma [1] A teratoma is tumor of germ cell origin, containing tissues from more than one ge germ cell line2. An immature teratoma is very rare tumor, representing 1% of all teratomas, 1% of all ovarian cancer, and 35.6% of all malignant ovarian germ cell tumors. It displays aspecific age,of incidence its usual in first two decaded rare afer menopause.toma contains immature elements unlike mature teratoma , an immature elements
Totipotent neoplastic cells can differentiate along the embryonal or extraembryonal lines.
- The embryonal somatic differentation along a primitive embryonic cell lines results in embryonal carcinoma.
- Extra embryonal differentiation along the trophoblastic line gives rise to choriocarcinoma.
- The yolk sac line give rise to yolk sac tumor (endodermal sinus tumor).
Immature teratoma in ultrasound appear nonspecific whereas at ct and mri predominantly solid with fat filled elements these patients of immature teratomaors are surgically staged via exploratory laparotomy with cytologic washings, peritoneal biopsies, an omental assessment (either biopsy or omentectomy) [3] laparoscopy is preferred mode in immature teratoma an immature teratoma contains varying compositions of adult and embryonic tissues. The most common component identified is the neuroectoderm [4].
Tumors may also present embryonic components such immature cartilageand skeletal muscleof mesodermal origin 5. Immature teratoma is composed of embronic endodermal derivatives [6].
Recently a reliable biomarker oct-4 are helpful in diagnosing malignant immature teratomas [7]
Thurlberg and schully devised a grading system on the basis of differentiation of the cellular element of the tumor The proportion of immature tissue elements defines the grade of maturity This was later modified by Norris etal who added quantitative aspect to the the degree of immaturity.
Grade 1 and2 usually have a normal karyotype Wheras GRADE 3 has abnormal karyotype.But, there may be still Be detectable alterations in gene level Treatment depends on fertility and grade Since the occurrence of immature teratoma is rarely bilateral, current standard of care is unilateral salpingooopherectomy with sampling of peritoneal implants [9]. Total abdominal hysterectomy with bilateral salpingo-oopherectomy are not indicated as they do not influence the outcome [10].
Fertility sparing surgery is the form of treatment in young patients10.zhao etal reported that here is no significant differences in survival rates or post operative fertility outcomes between two.
Aims and Objective of The Study
The aim of the study is to analyse the clinocopathological and survival outcome 10 cases of immature and mature teratoma associated with malignancies.
Material Methods
The case included-
- HPS confirmed immature teratoma and teratoma and immature teratoma with malignancies after staging laparotomy.
- HPS confirmed cases of teratoma.
Statistical Method of Analysis
Chi square test and Kaplan meyer survival analysis.
Descriptive Statistics – Total no of cases takenfor analysis is 10. immature teratoma alone3(30%),immatureteratoma with malignancies 3(30%) and teratoma with malignancies 4(40%). Table1immature teratma asocited with malignancies were one with yolk sac component, one with melanoma and one with embryonal carcinoma
An Immature Teratoma with Neuroepithelium, Yolksac and Embronal Carcinoma
The median age is 34 years with a minimum twelve and maximum 60 years Table 2. The follow up was a upto 60 months, minimum was 12 months. allthe the three cases f malignancies were followed up.
The case with a endodermal component presented the second year and the one with embryonal component in the 3rd year and the one with melanomain the first year.
The markers considered were ldh, bhcg,. Ldh was >400IU in 8(80%) and less <400IU in 2(20%) table 3.beta HCG<1Miu in 3(30%), beta hcg>1Miu(70%) table 4. The low grade 7 (70%) cases and high grade 3(30%) table 5The treatment was basically two groups. Conservative surgery group i.e unilateralsalpingoopherectomy7(70%), radical surgery group i.e b/l salpingooopherectomy 3(30%) table 6. There were 8 (80%) in stage 1a and one in stageIII (10%)table7 and one in stage 1c2(10%). The cases of immature teratma associated with ther malignancies i.e embryonal, yolk sac cmpnent and melanoma received adjuvant ct 6 cycles. Whereas the four teratoma with squamous cell carcinomas and those with immature teratomas alone i.e 4 cases without adjuvant were followed up.
The case with immature teratma associated with embryonal carcinoma presented in stageIII, The ther two cases of immature teratoma associated with endormal sinus and that with maelanma presented instage ic2 and stage1a respectively. The four cases teratoma with squamos cell carcinoma presented in stage 1a.and the three cases imaature teratoma alne presented in stage 1a
Cross tabulation analysis done of the individual factors i.e grade, stage, markers (ldh.bhcg),type of surgery ,with histology using the pearson chiquare and likehod ratio. Each factor analysed with three histolgical groups i.e immature teratma, immature teratoma with malignanciesand teratoma with malignancies the only significant assciation was that f type f suregery with the three grups with a p value-.007.
Survival analysis
Overall survival of immature teratoma is 66.7% with 95% confidence interval (.706, 1.000). The immature teratoma assciated with malignancies are divided into two categories the total survival in case of immature teratoma with associated is ther maignancies 66.7% with CI (.300, 1.000) total survival in case of immature teratoma with other malignancies is 33.3% with CI (.0673, 1.000). The cases teratoma associated with squamous cell carcinoma had no disease recurrence and all the 4 cases had survived
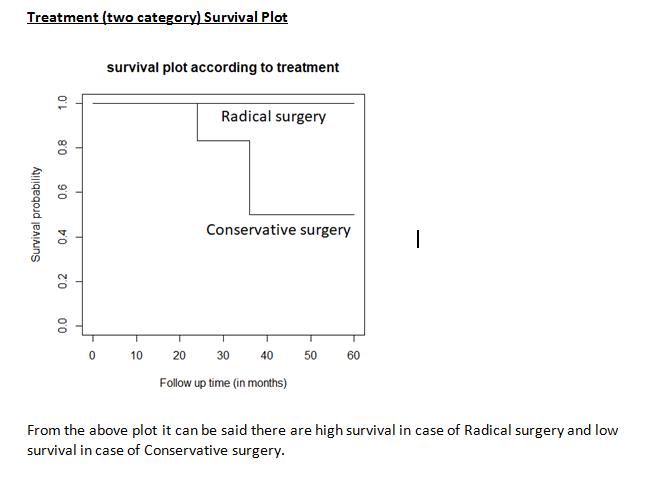
The total survival in case of Conservative surgeryis 50% with CI (.225, 1.000); which means there are almost 50% survival in case of Conservative surgery. There is no death event happened in case of Radical surgery so survival cannot be estimated in such .case
Results
Here it can be observed that the overall survival of immature teratoma is 66.7% with 95% confidence interval (.706, 1.000). The total survival in case of immature teratoma with associated is ther maignancies 66.7% with CI (.300, 1.000). In other hand the total survival in case of immature teratoma with other malignancies is 33.3% with CI (.0673, 1.000). this variability in the two groups of immature teratoma associated with malignancies is probably due two type of asscciated malignancies i.e embryonal and yolk sac and melanoma. The cases teratoma with squamos cell carcinoma all survived. Chi-square test on histology, shows there is no significant difference of survival pattern between different histology types at 5% level of significance. Among total 10 cases, there are 7 cases with low grade and 3 cases with high grade carcinoma. One death can be observed in the low-grade category where as in high grade category there are 2 death cases. The total survival in case of low grade is 85.7% with CI (.633, 1.000). The total survival in case of high grade is 0.01%; which means there are very low survival in case of high grade carcinoma. Among total 10 cases, there are 6 cases with Conservative surgery and 4 cases with Radical surgery. 3 deaths can be observed in the Conservative surgery category where as in Radical surgery there is no death case. The total survival in case of Conservative surgery is 50% with CI (.225, 1.000); which means there are almost 50% survival in case of Conservative surgery. There is no death event happened in case of Radical surgery so survival cannot be estimated in such case. From the above survival plot it can be said there are high survival in case of Radical surgery and low survival in case of Conservative surgery.Thus, there is no significant difference of survival pattern between different treatment types at 5% level of significance (p= 0.2).
Conclusion
The median age of presentation was 34 yrs although the lowest age being 12yrs to uppermst age 60 yrs. Maximum nos case of immature teratoma were low grade and early stage. The immature teratma associated with malignancies were higher grade.The The conservative approach was preferred in early stage and low grade .The overall survival of immature teratoma is better than overall survival of immature teratoma with malignancies. The type of associated malignancies i.e yolk sac and embryonal cmponent can differently affect the survival. Teratoma with squamous cell carcinoma has a good survival in early stage The low-grade type has better survival. The radical surgery group shows a better outcome.
The rarity of such cases, and early age of presentation prompted us to analyse there clinicopathlogical and survival factors. So, that it could be of help to others in deciding the radicality of management on the basis of the above factors.
- Sun H, Ding H, Wang J, Zhang E, Fang Y, et al. (2019) The Differences Between Gonadal and Extra-Gonadal Malignant Teratomas In Both Genders And The Effects Of Chemotherapy. Bmc Cancer. 19: 408.
- Nci Dictionary of Cancer Terms (2011) National Cancer Institute.
- Damjanov I (2009) Pathology Secrets (3rd Edn) Philadelphia, Pa: Mosby/Elsevier.
- Jump Up To:A B C Ulbright Tm (2004) Gonadal Teratomas: A Review And Speculation". Advances In Anatomic Pathology. 11: 10–23.
- Schmidt D, Kommoss F (2007) Teratoma of The Ovary. Clinical And Pathological Differences Between Mature and Immature Teratomas]". Der Pathologe(In German) 28: 203–8.
- Alwazzan Ab, Popowich S, Dean E, Robinson C, Lotocki R, (2015) Pure Immature Teratoma of The Ovary in Adults: Thirty-Year Experience of a Single Tertiary Care Center". International Journal of Gynecological Cancer. 25: 1616–22.
- Coran Ag, Adzick Ns (2012) Pediatric Surgery (7th Ed.). Philadelphia, Pa: Elsevier Mosby. 539–48.
- Jump Up To:A B C D E F G Di Saia Pj, Creasman Wt (2012) Clinical Gynecologic Oncology(8th Edn). Philadelphia, Pa: Elsevier/Saunders: 329–56.
- Ki Ey, Byun Sw, Choi Yj, Lee Kh, Park Js (2013) Clinicopathologic Review of Ovarian Masses in Korean Premenarchal Girls". Int J Med Sci 10: 1061-7.
- Jump Up To:A B Malkasian Gd, Symmonds Re, Dockerty Mb (1965) Malignant Ovarina Teratomas. Report Of 31 Cases". Obstetrics And Gynecology 25: 810-4.
Table 1
Table 1: Histology Table 1
Table 2

Table 2: Age and followup interval
Table 3
Table 3: LDH
Table 4
Table 4: BETA_HCG
Table 5
Table 5: All the three cases of immature teratma with malignancies presented in higher grade.The other cases of immature teratoma and teratma associated with squamous cell carcinoma presented in lower grade
Table 6
Treatment Table 6
Table 7
Stage Table 7
Table 8
Treatment * Histology Crosstabulation
Table 9
Chi-Square Tests
a. 6 cells (100.0%) have expected count less than 5. The minimum expected count is 1.20.
Table 10
Grade * Histology Crosstabulation
Table 11
Chi-Square Tests
a. 6 cells (100.0%) have expected count less than 5. The minimum expected count is .90.
Table 12
stage * Histology Crosstabulation
Table 13
Chi-Square Tests
a. 9 cells (100.0%) have expected count less than 5. The minimum expected count is .30.
Table 14
LDH * Histology Crosstabulation
Table 15
Chi-Square Tests
a. 6 cells (100.0%) have expected count less than 5. The minimum expected count is .60.
Table 16
BETA_HCG * Histology Crosstabulation
Table 17
Chi-Square Tests
a. 6 cells (100.0%) have expected count less than 5. The minimum expected count is .90.
Table 18
Status * Histology Crosstabulation
Table 19
Chi-Square Tests
a. 6 cells (100.0%) have expected count less than 5. The minimum expected count is .90.
Table 20
Table 21
Table 22
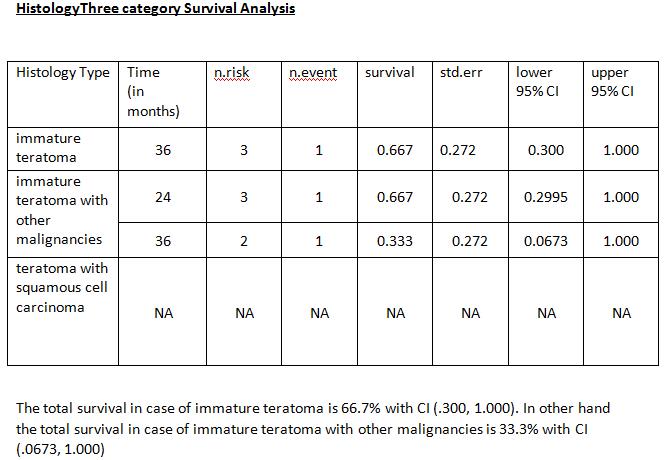
Table 23
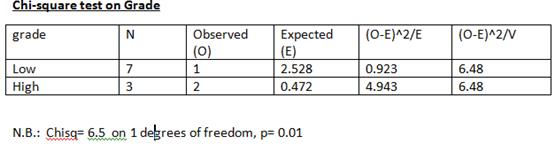
Table 24
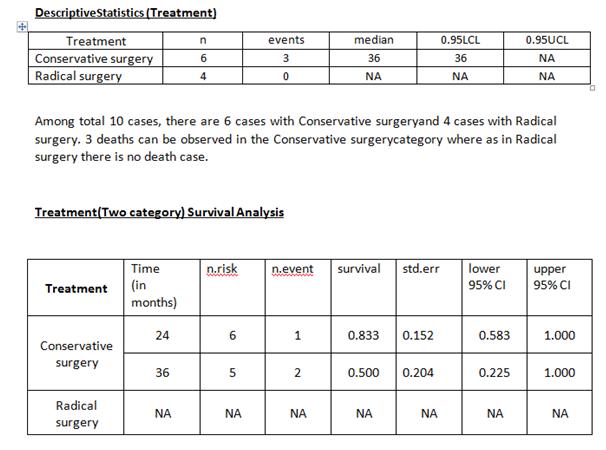
Table 25
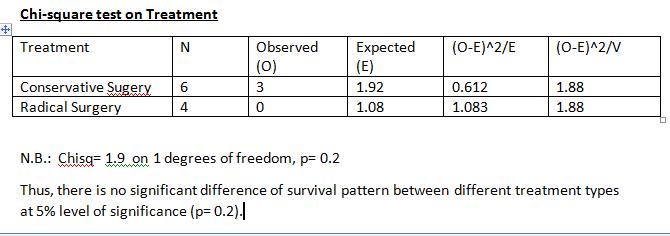
FIGURE 1
.JPG)
.JPG)
.JPG)
.JPG)
.JPG)
FIGURE 2
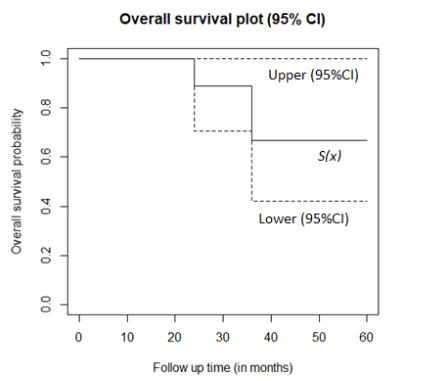
Figure 2: Over all aurvival Probability
FIGURE 3
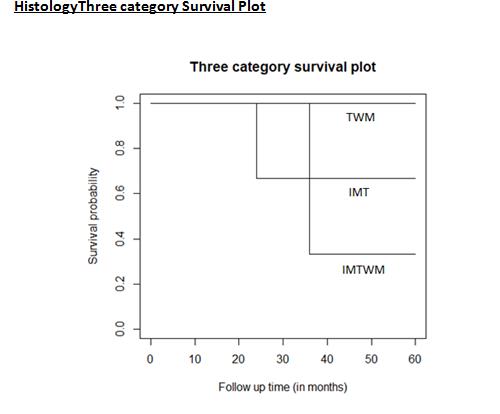
Figure 3: Overall survival analysis of the three groups i.e immature teratoma(imt), teratoma with bmalignancies(twm), immature teratoma with malignancies(imtwm)
FIGURE 4
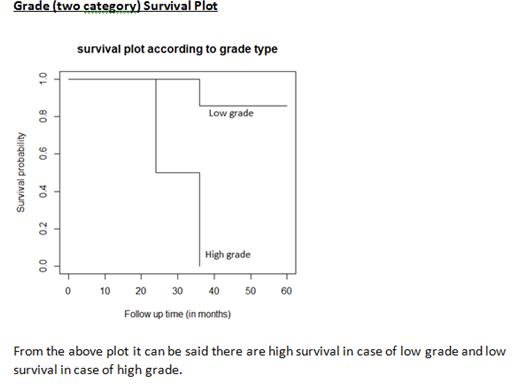
Figure 4: Grade Survival Plot
FIGURE 5
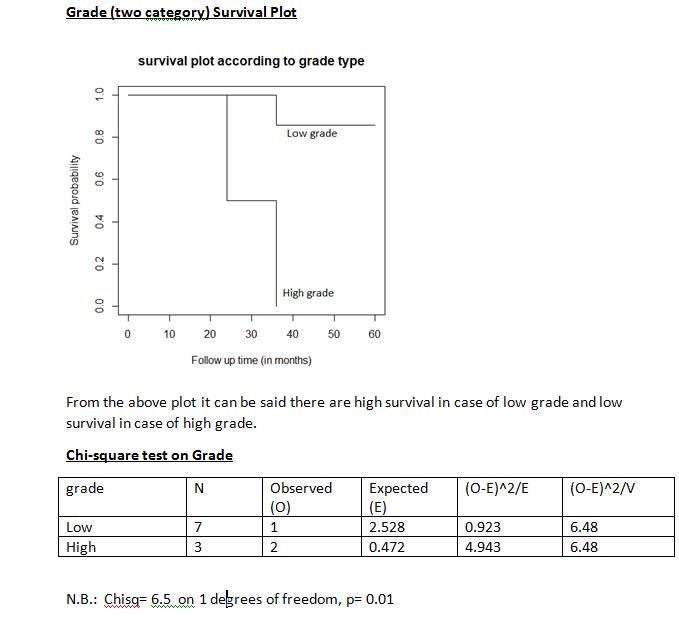
FIGURE 6
Tables at a glance
Figures at a glance