Neurophysiological Treatment of Neurological Disorders: By means of the Tomatis Music Listening Therapy
Received Date: July 03, 2021 Accepted Date: August 03, 2021 Published Date: August 05, 2021
doi: 10.17303/jnnd.2021.9.105
Citation:De Voigt MJA (2021) Neurophysiological Treatment of Neurological Disorders: by means of the Tomatis Music Listening Therapy. J Neurophysiol Neurol Disord 9: 1-25.
Abstract
Evidence is presented that the Tomatis Music Listening Therapy provides significant improvements of severe neurological disorders. This neurophysiological method stimulates effectively, via the hearing organs, the neurological system, i.e. the brain with its neuroplasticity. Independent Quantitative Electroencephalogram (QEEG) measurements, Brain Maps (BM) and Auditory Evoked Potentials (AEP), correlate with the listening tests (audiograms), therefore validating the therapy. This method consists of series with half hour sessions listening to predominantly, specially adjusted and filtered, W.A. Mozart music and Gregorian Chants (by the Abbey of St. Pierre de Solesmes, France). The diagnosis is mainly based on a listening test and anamnesis and in the present cases also on the independent QEEG measurements. The same procedure is repeated during the therapy after about 12 days (~100 sessions of ½ hr.) and at the end of the therapy (up to 5 times 5 days of ~180 sessions). This facilitates to observe the correlation between the two different measurements along with the resulting effects, which contributes to the validation of the method. The adjustments of the specially designed equipment depend largely on the interpretation of the listening tests and also on the observations of the client by the qualified therapist. The special headphones also with a bone vibrator on the skull enables to stimulate the bone conduction of sound to the ears to activate the internal communication or self-consciousness while the ear phones stimulate the communication with the outside world. Adjustments of the left / right balance would influence the activation of the right / left hemispheres with their different functions. Therefore the QEEG measurements enable to monitor the changes in the brain functions as well as the listening tests would show for the left / right ears.
It is nowadays generally accepted in the medical society that music stimulates both the physical and psychological conditions of patients. The present work illustrates that the Tomatis Listening Therapy, largely based on Mozart music, is even more effective and much more powerful than plainly listening to music. The present article describes 5 clinical cases obtained at the Mozart-Brain-Lab (MBL, Belgium) and at the Listening center , The Netherlands.
Keywords:Tomatis listening therapy; QEEG; Brain Maps; AEP; Stroke; Autism; Asperger; Dyslexia; Speech; communication
Introduction
The Listening Therapy is a training of the neurophysiological system by listening to specially filtered music. The positive influence of music on the brain has by now been well established scientifically and was long ago explored by the innovative theoretical and experimental work of the French ENT doctor professor Alfred Tomatis [1].
This Neurophysiological training has proved to be very effective in the treatment of neurological disorders such as autism, ADHD, dyslexia, brain damage, hearing problems, dizziness, and problems with learning, behavior, concentration and communication. In all these problems the central nervous system, for which the ear is the strongest entrance, particularly to the brain, plays an important role. The physiology of the ear, by movements of membranes, ossicles and muscles and transport processes also in the cells, produce electrical signals in the neurological systems, particularly to the brain. The APP Listening Therapy is based on hearing (Audio) and reproducing vowels and consonants (Phonology), as a result of which also Psychological changes take place, thus effectuating improvement of the problems. The resulting effects are excellently monitored by the listening tests and independently from the method by QEEG measurements, BM’s and AEP’s as presented below.
Of the rich scientific evidence of positive effects of music on our brain we refer to two standard works [2, 3]. An overview of the literature, concerning the efficacy of the Tomatis method is published by Gerritsen [4]. A first publication of our results concerning the correlation between the listening test and the QEEG BM and AEP can be found in [5]. This was part of the scientific validation of the method. The method with many results and cases, including those in literature is also contained in our textbook, [6].
The neurologist Oliver Sacks [2] applied music in various ways in his various neurological treatments such as Parkinson, aphasia, Alzheimer, Gilles de la Tourette etc. He obtained international fame with his treatment and description of the sleeping syndrome; “Awakening in Bewilderment”. It illustrates that our brain is excellently dedicated towards music, which may provide significant therapeutic possibilities for all kinds of neurological disorders. The book of the psychiatrist Norman Doidge [3] contains a full chapter devoted to the Tomatis Listening Therapy. It describes good results by applying the Tomatis method in the Centre at Toronto [7], nearby the place where Norman Doidge lives. There filtered Mozart music was considered “musical medicine using the special sound energy to form a bridge into the brain, to speak its language”.
The Tomatis APP Listening Therapy works in such a way that it influences the brain, which is also promoted by the neuroplasticity of it [8]. The training is based on the fact that the ear is the most sensitive entrance to the central neurological system, i.e. a large part of the brain, the vestibule-cochlear nerve, the vagus nerve and recurrent nerves. The sounds, after filtering, are presented to the two ears by a headphone as well as to the skull by a bone vibrator. In addition to frequency filtering, the various intensities and delays which operate differently on air and bone conduction are also adjusted. The processed sounds stem mainly from Mozart concerts and Gregorian chants. Tomatis has developed specific electronics which have been utilized and further elaborated at the Mozart-Brain-Lab (MBL) in Sint-Truiden, Belgium [5, 6]. Prof. Tomatis, a medical specialist in hearing, developed the method and conducted most of the research from the 1950’s on up to his death in 2001. He discovered the great psychological and physical influence the ear has on our functioning, communication, learning, language and speech, [9, 10, 11, 12] . His research with many experiments yielded a device called the “Electronic Ear”, later the Mozart-Brain Activator (MBA), which have been successfully applied in therapies all over the world. Statistics show long-lasting improvements in about 80% of those treated, as obtained from investigations in many institutions all over the world [4].
Independent replication was possible since the introduction in 1995 [13], at the Atlantis Institute in St.-Truiden of QEEG-based BM’s and AEP’s to analyze the initial situation of the brain of a client as well as the condition during and after therapy, in combination with the Tomatis Listening Therapy. They can be correlated with changes in the listening tests and with the observed improvements of the problems of the individual subjects [5]. A wealth of data is available internationally and also at the MBL institute at Sint-Truiden, Belgium of which five examples are presented below.
From the many publications of the 1980’s and 1990’s the relation between learning, language and speech problems with listening becomes indisputably clear [14-17]. This follows from the EEG measurements on groups of test persons with and without those impairments. The measured AEP’s indicated a reduced activity of the left hemisphere in the group with impairments as compared to normal subjects [5, 13].
Dichotic testing has been carried out, where the two ears are offered different sounds. The right ear normally proves to be dominant, especially in the short term. It is concluded that the left hemisphere is especially equipped for the fast processing of phonological and linguistic processes. With rapidly changing stimuli the left frontal cortex is especially activated at the center of Broca. This auditory lateralization was found stronger in men than in women, which is probably the reason that more dyslexia occurs in boys than in girls. With those disabilities the phonemic (sound entity) neural representation shows impairments. Children with speech impairments and dyslexia show problems especially with rapidly changing sounds, due to the reduced activity of the left hemisphere.
Microscopic studies also in the 80’s and 90’s of dyslexia and aphasia (incapacity to speak) showed that brain tissue in the lateral corpus geniculate (sensory switch station in the Thalamus) was less ordered and that the cells were generally smaller than in the case of normal subjects. This can cause the slower visual processing. Also a less active left hemisphere was observed. As a cause for this a disturbed sensory (auditory) input in the first development stages of the child was mentioned.
It is interesting that above scientific neurological investigations confirm the propositions that Tomatis made some 40 years earlier. Moreover the results of acoustic treatment in the 1980’s and 1990’s seem to agree with those of Tomatis, introduced decades before, and which are nowadays applied everywhere in a strongly improved form.
The five cases discussed below illustrate the method and comparison of the listening tests with the independent QEEG data prove the progress reported by the subjects or by their relations.
Materials and Methods
The method, procedures, equipment and results are extensively described in our textbook [6]. Therefore we will summarize here only the main features.
Diagnostics; the listening test
The starting point of the therapy is the listening test, which consists of an audiogram, interpreted both physically and psychologically by a trained APP consultant. This is executed with a common audiometer, but with a so-called Tomatis calibration. An ideal curve is given in figure 1 which, according to Tomatis, reaches a maximum sensitivity in the communication (speech) region of 1000-3000 Hz, similar to the known auditory spectrum. This test indicates possible problems in certain frequency regions in bone and/or air conduction for the left or right ear, so consequently the right or left hemisphere respectively, mostly relating to the different brain functions. The latter phenomenon is based on the notion that contralateral connections between the ears and the hemispheres are stronger than the ipsilateral ones. A high bone conduction in relation to the air conduction signifies that the subject is dominantly listening to him/herself, thus living in his/her own world and poorly controls the communication with his/her surroundings. One can experience this phenomenon during speaking that one hears oneself mainly via bone vibrations of the skull, therefore listening to oneself. Localization errors are registered if the other ear than the tested one perceives the sounds. This may signify confusion in orientation and between emotion and rationality. The discrimination between tones, or selectivity, is measured between adjacent frequencies in the listening test. A closed selectivity signifies psychological screening from the outside as a kind of protection. The ear (auditory) dominance, or laterality, is measured as an indication that the subject is more or less emotionally or rationally oriented (Figure 1).
The results of these tests are analyzed by a qualified consultant to observe both physical and psychological factors. Three zones of frequency are relevant; The physical Zone I, 125-1000 Hz, the communicative Zone II, 1000-3000 Hz, and the spiritual, Zone III, above 3000 Hz. Overall, one may distinguish three pathological types: (i) the physical type with a decreasing curve, where the low tones are more strongly present than the higher ones. There is also a decrease in the communication zone II and in the spiritual area zone III. This is generally accompanied by depression. (ii) The rational type with a maximum in the middle frequency area, zone II. This type shows a notably dominant behavior and in case of an extreme form can take the attitude of paranoia. (iii) The intuitive type shows a rising curve with a maximum towards the high tones. It lacks a positive body image and proper communication. A serious form is schizophrenia and can lead to suicidal tendencies.
The bone conduction is an indication of how one looks at him/herself, or inner listening. It also signifies the self-confidence, the tensions and the weaknesses of the personality. The air conduction signifies the communication with the outside, or listening to the outer world. Ideally the air conduction must be located somewhat above the bone conduction (according to the Tomatis calibration of the audiometer) to have a good control to the outside world with the inner possibilities and potential.
The right ear (therefore the left hemisphere) is indicative of rationality, verbalism, the present and the possible relation with the father. The left ear, on the other hand, is indicative of emotionalism or feelings, imagination, orientation in space and time, the past and the possible relation with the mother. The left ear (right hemisphere) represents the human being as a total, whereas the right ear (left hemisphere) indicates how its capacities are used.
Zone I is indicative of the body posture and the motor performance. This means both gross and fine motor functions. Here our body image manifests itself. Here the structures of rhythm, space, time and order can be analyzed, structures which are also the key competencies for rational thinking and mathematics. Zone II is essential for language and communication. This is also the area of control relating to voice and music. The key information for language is contained particularly in the vowels characterized by the formants as the sound images of it. Those formants 2 and 3 are localized in this zone (formant 1 is situated in zone 1). Zone III is important for brain dynamics, cognition, spirituality, creativity and intuition, seen in the increasing or decreasing air conduction. The overtones or harmonics, which mainly fall in this frequency range, determine the quality or color of voice and music.
There are three more factors to analyze: Laterality is the dominance of the right or left ear.
The right ear is our neurologically fast ear to communicate and enable the voice to utilize more harmonics. Left or not lateralized indicates a slow perception response. The natural switch in early childhood of the dominant left ear to right ear mostly occurs between the 7th and 10th year. Selectivity is a measurement of the discrimination of adjacent tones. A closed selectivity means that one cannot distinguish adjacent tone differences. Apart from a bad communication with and poor perception of outside signals, this is also some sort of self-protection, as an emotional curtain. In that case one is more an observer than participant. The natural opening of the selectivity, which is normally closed in early childhood takes place around the 8th year. Spatiality means the correct perception in the proper ear. Mistakes in spatiality point to an erroneous exchange between the left and right ear, both in air as well as in bone conduction. Spatiality errors indicate special orientation problems and confusion, particularly between emotional and rational aspects, both towards him/herself as well as towards the outside world. They may also indicate stress in functioning at the corresponding frequencies.
As far as resonance of sound in the body is concerned, the high tones will especially address the head, the middle tones the breast and low tones the belly and the lower part of the body. Tomatis has empirically determined the relation between peaks and scotomas at certain frequencies and physical disorders of the spine or organs. That is for example a peak at 1000 Hz in the bone conduction and a scotoma in the air conduction indicates a possible problem in the stomach.
Irregularities in the curves may indicate physical disorders as well as psychological problems. A sag in the curve (also called scotoma) therefore means diminished listening sensitivity that indicates a weakness or a shortage, which frequently asks for compensation. A significant example of a scotoma in the middle frequency area (zone II), where vowels and consonants are formulated, may be indicative of dyslexia, communication problems, or language development impairments. Generally irregularities in the curves indicate mental or physical blocking. A peak, on the contrary indicates over-reacting, caused by some problem in the body at the corresponding frequency.
Diagnostics; QEEG measurements
In contrast to the classical EEG, in a QEEG the data are processed quantitatively to generate a map of the brain, where the intensity of the frequency bands (delta, theta, alpha, beta) are displayed over the brain surface, called the brain map, like a temperature map. At the Atlantis institute 19 electrodes were formerly used, with Sirius ESAOTE BIOMEDICA equipment on the skull, according to the International 10-20 System of electrode placement. Thereafter the new COGNITRACE (ANT) equipment has been introduced, also with 19 electrodes. The standard “eyes closed condition” was being used as well as “eyes open”. Unwanted “noise” was removed in standard mathematical procedures. Each brain wave has a certain frequency. According to international standards, 4 groups are distinguished:
Very slow waves: δ 1-4 Hz; like in sleeping
Slow waves: θ 4-8 Hz; like in dreaming
Fast waves: α 8-12 Hz; like being alert
Very fast waves: β 12-32 Hz; like activity/aggression
For instance, in the case of poor alertness one observes little α (alpha) and β (beta) activity and/or much δ (delta) and θ (theta) activity. The maps are also age dependent, i.e. for young children <6 yrs. one mostly observes dominant delta (mainly 3, 4 c/s) and theta (mainly 5, 6 c/s), but for ages >6-7 yrs.: alpha becomes dominant (8-12 c/s) with a posterior (occipital) maximum. From the age of 2 on the alpha activity starts to develop. For learning and language activities the left temporal hemisphere is particularly important.
Measurements of AEP’s
At the Atlantis Institute Auditory Evoked Potentials (AEP) are measured with the same equipment as for the brain map. Auditory clicks or tones are presented to the ears and the measurements are registered [13]. The brain responses to all electrodes are recorded separately and then grouped together as functions of time in milliseconds. The time domain of the first 10 msec relate to functions of the lower brain stem and are an objective measure of peripheral hearing in very young or uncooperative children. The middle latency (10-50 msec), the long latency (50-100 msec) and the cognitive auditory potentials (100-700 msec) relate to functions of the higher brain stem, the temporal primary cortex and to the frontal association cortex, respectively. Deviation of the middle latency potentials from normal patterns is indicative of problems with consciousness, attention mechanisms and of the processing time of the central auditory system. Language development disorders show up as deviations in the middle latency auditory potentials, particularly in the temporal complexes, the T4 (right) and T3 (left) positions.
The most important thing is to measure the different amplitudes (e.g. the one of N200, negative potentials after 200 msec.) under two conditions for a certain individual, performed under both the attention (to the rare tones) and non-attention condition. An electrical negative response appears 100 msec. after the tones, (N100), at which time the subject’s attention is directed to the task. The N100 intensity should increase as a function of early selective attention. Two hundred msec. after the rare tones an electrical negative response appears (N200), even when the subject is not attentive. This is a measure of automatic discrimination. Three hundred msec. after the rare tones, in the attention condition, an electrical positive response appears (P300) and this is a measure for controlled meaningful stimulus processing. These measurements are also carried out with the eyes closed and are known as the “odd-ball paradigm”. The deficiencies may show up as a weaker potential and/or a prolonged latency time.
The new equipment, also with 19 electrodes came with a validated BEAM database of control groups with normal or statistically standardized subjects of all ages. The measurements are nowadays carried out with the eyes closed as well as with eyes open. From the various projections, i.e. left, right, top, front and back, a case is presented below with only the left, right and frontal brain maps. Here the measurement was the eyes closed condition, for δ, θ, α, β maps of the subjects along with those of the comparable standards and the differences between the two of them. The latter deviations are quantitatively expressed in Z-score or standard deviation in microvolts squared, indicated by the small vertical bars in each left upper corner (see e.g. figure 5). The extra cortical activity as compared to the control group is indicated by the red color in the brain maps. The result is considered to be comparable with the control group if the standard deviation does not exceed ±2.
Execution of the therapy
The procedures of executing the therapy are extensively described in various publications [1, 5, 6, 12, 18] Here we will summarize the main phases. Based on the results of the listening test, an individualized Listening Therapy plan is constructed. This includes, in most cases, certain filtered music, the mother's voice and the individual's own voice. Always a processing whereby a continuous, but irregular, alteration between filtered low and high tones is provided. This alteration promotes the Tomatis effect, whereby the voice produces the frequencies that the ear can hear. Here the high tones act as stimulation and the low tones as relaxation. The basic sound material is that of Mozart’s concerts (with about 110, sometimes combined, pieces available at the Tomatis institutes, mostly violin, piano and flute), which are known for their great harmony, high rhythm, and large density of high frequencies, and which provide a feeling of universality [19]. Therefore they provide great cortical stimulation as well as positively influencing physical aspects [20]. Also Gregorian chants (with about 30 pieces available, both voices of nuns and monks) are used to deliver sufficient training of the body coordination because of the low rhythm and quietness. They cause also quietness in case of too strong reactions and balance of the parasympathetic system because of those properties.
The therapy starts with a passive phase of unfiltered music, followed by a long phase of highly filtered music, up to 6000-8000 Hz, followed again by unfiltered music, on both the ears and skull.
Particularly for young people, and those with early youth or psychological trauma’s, also the mother’s voice is recorded and used in the high filter phase. The use of the mother's voice appeared extremely important. This is due to the fact that one returns unconsciously to the fetus time. This may have a strong psychological effect and after the sonic birth by removing the high filter one may resolve or weaken the past traumas or development disorders. The therapy is concluded by an active language phase using the client’s own voice with reading and singing. The therapy is executed uniquely in qualified center’s with specially developed electronics. Generally, the sounds for the Listening Therapy are provided in a first cycle of 8 to 16 days with 2 to 4.5 hrs. of listening and with two interruptions of 1.5 hrs. in the latter case. After an interval of about four weeks the next cycle is about a factor two shorter in days and more of the same cycles follow with somewhat longer intervals. At the beginning of each cycle, a listening test is conducted to check the changes and to adapt the program. The total duration of the therapy depends on the subject's problems and on his or her response to the treatment, but consists in most cases of at least three short cycles after the first long one, when the problem is not too deep. Therefore, potential clients should be prepared for this intensive and time-consuming therapy in order to obtain the motivation necessary for positive results.
Electronic equipment for the APP therapy
The equipment exists in the form of an original Electronic Ear, now replaced by the Mozart Brain Activator (MBA) which has connections to a music player, to a microphone and ear-phones with skull vibrator. These are fed by a cassette recorder, CD player or other recorders such as the specially developed player APP501 with a hard disk at MBL [6]. The cassette tapes, CD’s or sessions on the APP501 are recorded with selected music and text for different languages with or without filtering. Most units originate from recordings carried out by Tomatis.
The Electronic Ear is an invention of Tomatis [1,12], processed according to the Tomatis effect whereby the switching frequency is adjustable and, if desired, also filtered with an adjustable low-pass or high-pass threshold on frequency. The adjustable filter can remain fixed during a session or slowly increase or decrease from and to certain frequencies, the highest being 8000 Hz. A particular property is the processing of the sound by passive and active electronic channels. In the passive channel the low tones, below 1000 Hz, are amplified and the high tones weakened. The active channel works in a reversed way, thus with amplified high tones and weakened low tones. The active channel therefore provides extra stimulation, whereas the passive channel relaxes. The switching between the active and passive channels always takes place continuously during the 30-minute sessions and is dependent of the adjustable volume levels. This is called the Tomatis effect, as discussed above. This process has its effect both on the bone and air conduction, with a fast change of the bone conduction and, after an adjustable delay (called precession), the air conduction follows. The Electronic Ear simulates in this way the functioning of the human ear with its latency delay and in this way it will correct its performance. The Tomatis effect results, among other things, in a kind of massage of the ear and especially of antagonistic muscles, or osteo-muscular gymnastics. Moreover other processes are also stimulated such as activation of the Corti-cells, the nerve system and the brain, therefore a neurophysiological training.
It should be noted that the original Electronic Ear was based on analogue electronics, whereas the newer development in the form of the MBA at Sint-Truiden utilizes digital electronics. This has been possible only because of the refinements in this field such as 24 bits storage and 96/192 kHz accuracy sampling. This enabled the significant sharpening of the filtering. The Tomatis effect can now be improved from a maximum of +- 18 dB in the old machine to the desired maximum of +-25 db. Moreover, new functions have been added, such as a variable commutation frequency between 500 and 3000 Hz, which used to be fixed at 1000 Hz. Also the transition between the two channels has been increased from 6 dB/octave to 12 or even 18 dB/octave, whatever is chosen. Besides the former high pass filter the MBA also contains an adjustable low pass filter.
The MBL APP501 storage system contains a hard disc to store music and voice (language) units. It works under Microsoft Windows and it is provided with an Ethernet connection to be served by another computer and so be connected with the internet. Here we will only present the main features. In fact the APP501 feeds the MBA therapeutic device. The device has a large storage capacity of 500 GB. It contains over 230 music units (30 minutes each) and 13 European languages with 530 pieces including some other languages like North-American. Other pieces can be added, particularly numerous mother’s voices, recorded via the MBA. The accuracy of 24 bits, 96 kHz, both for recording and playback is sufficient to apply digital electronics and to compete favorably with analogue electronics.
Results
5 Cases
Case I: Erhardt, Brain Damage
The man was born in 1960 and suffered from a severe stroke in 2003. He lost his speech completely (aphasia). He walked badly, particularly his right leg did not function and experienced severe general locomotion disorders. Regular treatment for about two years, like physiotherapy, only resulted in marginal improvements.
In 2005 he started treatment at Atlantis in Sint-Truiden, as described in the textbook [6]. The first listening test in 2005 is presented in figure 2. A large scotoma appears at 750 Hz R-ear, indicating brain damage L-hemisphere! The recorded brain map indeed confirms the lesion present in the left hemisphere (see figure 4). This must cause locomotion and speech disorders. Large irregularities are present in the communication area at 1000-3000 Hz, indicating poor speech and lack of language application. Above 3000 Hz also large irregularities, i.e. lack of intellectual performance, with the bone conduction above the air conduction indicating lack of control. The total curves R-L are very non-harmonic, indicating poor coordination between the two hemispheres (Figure 2).
On the basis of this test and the anamnesis a special listening program was offered, according to the Tomatis method. This consisted of 424 30-minute sessions in total, lasting 2½ years, with 9 cycles of 5 to 12 days each, with 2 to 9 month’s intervals. First unfiltered Mozart music (various pieces out of the ~110 available) and Gregorian chants (various pieces out of the ~30 available) were applied and thereafter a high-pass filter at 6000 Hz. The therapy ended with unfiltered music and practical speech and singing exercises with the microphone, utilizing the mother tongue and Gregorian chants.
The last listening test in 2008, given in figure 2, shows that the large scotoma at 750 Hz R-ear has disappeared as well as the large irregularities in the communication area at 1000-3000 Hz and above 3000 Hz. This means that the disorders related to the brain damage must have disappeared or diminished significantly, with returned speech, communication and intellectual performance as well as better locomotion control. Indeed the total curves R-L are now much more in harmony, indicating better coordination between the two hemispheres. However, remnants of the brain damage still show up in the R-ear where the bone conduction at 250 Hz is slightly above the air conduction, indicating still some locomotion problem. In the L-ear the air conduction at 6000 Hz shows too much decrease, still referring to the old problem in the upper part of the head. Also the localization errors in the bone conduction indicate that some coordination problem still exists (Figure 2).
The first QEEG data are presented in figures 3 and 4, using the Sirius equipment. The findings from the listening tests are replicated by the QEEG data, taken at the same time as the listening tests. The cognitive AEP’s (figure 3) only show a clear N100 potential and perhaps little P300. This indicates the absence of controlled meaningful stimulus processing. The brain map in figure 4 indicates the very strong δ activity and the θ activity frontal and in the β map the damaged lesion area is seen left temporal. Moreover, the α activity is asymmetric. All these features correlate with those observed in the first listening test of figure 2.
The last QEEG data are given in figures 5 and 6 taken with the new COGNITRACE (ANT) equipment, also employing a database of control groups, which enables comparison of the subject with a standard. The very small Z-scores (Max / Min upper left corners), varying between 1.04 and 1.64 for the θ, α and β activity, resemble a normal situation. The result is considered to be within the normal range of the standard deviation. Only the δ score with Z=4.05 still indicates a remnant of the lesion area left temporal and frontal, as can be seen by the red color in the difference maps. The eyes-open maps are consistent with the eyes-closed ones (Figure 5).
Part of the QEEG cognitive AEP’s for the electrodes Fz, Cz and Pz after the therapy in 2008 are presented in figure 6. Most of the AEPs are present, particularly the attention potential P300(2) with the rare tones (red curves) as can be seen in the table to the right of the potentials. The controlled meaningful stimulus processing is now clearly present. The Fourier transformed spectrum P3-P4 in the case of the rare tones is particularly strong as compared to the frequent ones. Also the reaction time of 303±84 ms is close to normal.
It can be concluded that both before and after Erhardt’s therapy the data of the listening tests correlate very well with those of the QEEG data. Indeed, Erhardt’s speech has recovered close to normal, although still a little slow. His locomotion is good now and he walks very well. Also his intellectual performance is almost back to the former level (Figure 6).
Case II: Freddy, an autistic boy
A 4½-year-old boy, Freddy, was born with deficits that resulted from oxygen shortage, was autistic, did not talk (analyzed at the University of Leuven, Belgium), was hyperactive and very aggressive. He suffered psycho-motor retardation, and language development disorders. Freddy was given intensive Listening Therapy at the Atlantis Institute, Sint-Truiden, Belgium for 1½ years [5, 6]. The therapy was executed at night, one period of 12 nights and one period of 10 nights during sleep, because he did not allow the headphone on his head.
Thereafter he could accept 3 more periods of 5 daytimes. The first somewhat reliable listening test exhibited a big difference between the bone and air conduction with strong and chaotic irregularities, consistent with Freddy’s problems (see Figure 7). The very high bone conduction, especially at the beginning, is typical of autism. Eighteen months later the test showed large improvements, although the bone conduction results were still a bit too high, but not uncommon at this young age (Figure 7).
In Figure 8 the QEEG-brain mapping data (as to delta waves) are compared before and after the therapy. The brain map before the therapy shows an asymmetry; the left electrical (negative potential) brain activity is much stronger than the right one. Also an asymmetry is seen in the amplitudes of the MLAEP’s with a dominance of the left hemisphere. With a stimulus to the left ear the MLAEP response left (T3-complex, broken line) was temporally much larger than right (T4, solid line), as can typically be seen in the case of language development disorders. Normally this test shows a symmetric T-complex or a reversed asymmetry (response temporally higher right than left). This imbalance was restored after the therapy, with even a stronger response on the right than the left. The Mason asymmetry index before the therapy was –0.64, which is typical of a language development disorder. After the therapy this index was restored to normal. These results are consistent with the progress of the listening tests in figure 7.
Freddy has experienced great progress in the 1½ years of intensive Listening Therapy. The boy has become quieter, with more concentration and better speech, he talks more fluently, and is less aggressive. He has become markedly alert and interacts with the outside world. These changes have been observed by the clinician and parents and have been documented by his progress in speech and communication with the environment, particularly at school.
Case III: Maurits, Syndrome of Asperger
A man, Maurits, 35 yrs. old, was treated at the Tomatis Listening Centre of Gorinchem, The Netherlads [6] and was characterized as follows:
The birth proceeded after pre-eclampsia, a placenta infarct, and also anoxemic (oxygen shortage). The Syndrome of Asperger was indicated by the neurologist. He showed spastic movements and coordination and concentration problems. He experienced a weak social acceptance, and no self-confidence. With hammer toes he walked badly. His speech was too fast, and he talked too much. Those aspects are consistent with Asperger.
The listening test in figure 9, taken at the beginning, show irregularities, particularly left. Also concentration and energy problems were noted at low frequencies with a higher bone conduction, so no body control and weak locomotion. The relatively low air conduction at low frequencies in zone I and the high bone conduction in relation to the air conduction (negative antennae) indicates weak behavior, therefore a frontal brain lobe problem (in the brain map in figure 10; indeed a strong frontal δ activity, hinders development of the α activity). In the communication area, middle frequencies 1000-3000 Hz, the irregularity leads to bad speech rhythm and the spatial errors (red dashes at the bottom) both left and right at low frequencies confirm the body confusion (stress in the body). The selectivity errors (dashes at the top) mean poor contact with the outside world, but also a kind of self-protection. This is considered as a psychological curtain to screen himself from the outside world (hatched area) (Figure 9).
The therapy was quite long and encompassed 34 sessions with Mozart and Gregorian, non-filtered, 12 sessions to reach the 6000 Hz filter, 87 session with the mother’s voice filtered, all with balance 70% left (care was taken with possible brain damage), 14 motor adjustment sessions (low tones, balance 100%) and gradient 12 dB/octave. After the acoustic birth (return to all, also low tones again) with many active sessions, reading, singing, also densified music with motor adjustments. The listening test II after 197 sessions (see figure 9) shows that the irregularities on the left side have been removed. The test has strongly improved, particularly the bone conduction in relation to the air conduction, both left and right. However, the curves are still slightly too flat, which indicates there is still tension in the body and bad concentration. However, the negative antennae (bone conduction high at 250 Hz) have disappeared, leading to less nervousness, being quieter, having better body control and improved speech. Also the air conduction has now reached a higher level, resulting in weakening the frontal problem. The spatial errors have disappeared, together with the body confusion. But the selectivity still remains closed, with the emotional screening and the resulting protection still present.
Those aspects are also correlated with the brain maps taken in Atlantis Sint-Truiden, Belgium and are presented in figure 10, for the beginning on the left side. A dysfunction is seen for the δ and θ waves left frontal, which are too strong for his age, confirming the poor behavior. Also an insufficient α rhythm is recorded, hindered by the strong δ activity. The Brain map at the end is also given in figure 10 on the right. It shows strong improvements, particularly the α rhythm is a factor of 3.7 stronger (see color scales) and activities are occipital. Also occipital a β lesion zone is seen, but this activity is a factor of 3 weaker than before (Figure 10).
The EEG time curves with indicated AEP’s at the beginning are given in figure 11 left. They show a flat or very weak spectrum, only the P100 appears weakly present but the other potentials seem absent. All parameters are consistent with intra uterus brain damage by anoxemia. The AEP curves at the end are also given in figure 11 on the right. Now the curves are closer to normal with pronounced P100, N100, N200 and P300. However, surprisingly, only the passive measurement seems to exhibit strong potentials and they are less pronounced when the subject listens actively to the clicks. This signifies that performance is weaker when attention is forced.
After a large part of this lengthy therapy the following results can be reported: He is quieter and the social environment reacts very positively. The parents as well as the friends have also noticed improvements in speech. He has a better concentration. He is clearer in the head and in thinking. He has more self-confidence and dares more; he has even obtained his driver’s license. He exhibits a better steering in hands while eating.
Case IV: Nike, Dyslexia
Nike, a boy, was born extremely premature in the 23rd week of pregnancy on 11-19-2007. This was the earliest birth they have ever heard of at the University of Koln. It deserved an interesting article in “Team F – „Erfahrungsbericht’’ (Experience report) with the title: “ Nike--eine Handvoll Leben” (Nike—a handful of life). During the three months in the incubator his mother paid lengthy attention with her recorded spoken word and singing, also when she was not present. This is exactly a favorably situation Tomatis has advertised for the fetuses. She could even serve the little boy with her breast, but after 5 month a probe in the stomach was necessary. After 9 months in the hospital he was allowed to go home. Mother provided 3 more years the breast on advice of a spiritual therapist. This should have developed a sort of ‘’arche thrust’’ and mother bonding. He visited a normal primary school, but with the assistance of a development therapist. However he showed great difficulties with learning. He was a child with dyslexia and reading and writing were extremely difficult for him. He visited the Atlantis Institute in 2016 at the age of ~9 years to start the Tomatis therapy (Figure 12).
The first listening test in figure 12 at age ~9 yrs. shows large irregularities, also in the communication area of 1000-3000 Hz of the left ear. This is consistent with dyslexia, speech and communication problems. Also the bone conduction (BC, red) is mainly above the air conduction (AC, blue), signifying loss of control and inner tensions as a refusal for spoken and written language. The auditory lateralisation is mainly behind (H) thus left, therefore ‘’sensitive emotional’’. The selectivity was totally closed, left and right. This means that he was living behind an “emotional curtain”, not taking part in what happens but only observing the outer world with bad discrimination of sounds as a result.
The last test, 3 yrs. later, shows several improvements. The irregularities are significantly less, therefore he blocks himself less. The bone conduction is now mainly below the air conduction, meaning more control to the outside world. This is particularly important in the region 1000-1500 Hz., because formant 2 is located there, important for all vocals. This is now easier to assimilate in the global emotional language (left ear, right hemisphere). The selectivity has opened now. This allows him to make a better discrimination of sounds, and being more awake. Also the laterality has shifted towards the (rational) right ear (Indicated by V front, instead of H) (Figure 12).
The improvements of the brain maps in figure 13 are consistent with those of the listening tests. Notably the Z-scores of the δ waves are diminished from 4,8 to 0,9 μV2. Also those of the β waves came down from 3,9 to 1,4 μV2.
The AEP’s in figure 14 exhibit the same improvements as the brain maps, taken with the same equipment. Notably the P3 after 348 ms in Cz and Pz mount to 24,4 μV, while they were absent or weak in the first measurement. Also some N1 in Fz and Cz shows up at 86 ms and P2, N2 in Pz at ~200 ms. This confirms that Nike has become more alert and responding to outside signals. Interesting are the red curves (with attention), which are too high at the beginning in the negative area of the three locations Fz, Cz, Pz. This is reversed in the last measurement, particularly for the middle and long potentials ( e.g. for P300) and those rare, attentive, responses are then larger than the frequent responses, which is important for understanding, memory and concentration.
In the period in between two early tests and brain maps Nike showed steady improvements. He appeared more lively, better concentrated and was able to read and write letters and simple words. During a dictation just before the second brain map he managed to fill a full page with dictated words, although those ending with a ‘’d’’ he wrote a ‘’t’’. However, the difference ‘’d-t’’ based on the rule of time lengthening was not known to him at the time, as was the case with the doubling of consonants. Nevertheless the words were clear with a good handwriting, an enormous progress in a relatively short time. It has become clear that Nike has improved markedly, indeed. His dyslexia has become less troublesome.
Case V: Rick, Communication , speech problem
Rick a boy, born 4-17-2012, came to the Atlantis Institute for a Tomatis therapy in 2019 at an age of 7 yrs. He experienced a late speech development, he still did not speak fully and changed between words and sounds. He also needed much sleep (Figure 15).
The irregularities in the later curves in figure 15, particularly right are less pronounced, therefore he should less block his speech. The distance between the high bone conduction (red) and the air conduction (blue) has changed. This is significantly improved at the high tones between 1000 and 4000 Hz. left, meaning a better emotional control in speech, better automatization, better understanding, better expressing. The laterality has largely changed from left to right, which indicates his rational steering rather than emotional of the communication. Although the listening curves are still far from ideal, the progress in this short therapy is much encouraging (Figure 15).
The Brain maps in figure 16 show significant improvements; particularly the δ waves came down from a Z-score of 23,3 μV2 to 9,6 μV2 in the latest measurement. Also the values for the β waves changed from 9,3 to 2,9 μV2. This means that he is less of a dreamer and more structured in activities. Altogether this seems remarkable after such a short therapy. Similar improvements are visible in the AEP’s of figure 17. Interesting are the red curves (with attention), which are too high at the beginning in the negative area of the three locations Fz, Cz, Pz. This is reversed or less pronounced in the last measurement, particularly for the middle and long potentials ( e.g. for P300) and those rare, attentive, responses are then larger than the frequent responses, which is important for understanding, memory and concentration.
In conclusion is the speech markedly improved, even after such a relatively short therapy. This is confirmed by others; relatives and school. He attends now a special speech school. He is still sensitive for sounds, but altogether he is more awake.
Discussion and Conclusions
The presented 5 cases show significant improvements, due to the Tomatis listening therapy, in the medical diagnostic data of QEEG as summarized below and some of them more extensively in our textbook [6]. The BM’s and AEP’s of the presented cases show main improvements particularly in communication and speech, in social and intellectual performance, in memory, locomotion and concentration, The generally observed tendencies of changes due to the Tomatis listening therapy are better communication, speech, language, concentration, social behavior, self-confidence and improved autism and dyslexia. Obviously the Tomatis method has its limitations in curing severe illnesses of the organs, muscles or senses, therefore physical disabilities such as inflammations, cancer etc., which should be referred to regular medicine.
The present cases out of many other treatments, where listening tests as well as a brain mapping were performed, have proven that the results of the listening test are reproduced by the QEEG data. This illustrates independently that the results of both methods correlate [5]. In most cases attention and concentration problems are observed in the Listening test by means of the high and often descending bone conduction at low frequencies compared to the air conduction test results. This correlates strongly with large δ activity frontal and prefrontal and with the absence of or weak α activity, mostly occipital, in the corresponding brain maps and with weak N200 and P300 amplitudes in the oddball paradigm AEP’s, both indicating little alertness. After the Listening Therapy those aspects have improved in the listening tests, as well as in the brain maps and AEP’s. Generally, in the case of language disorders a correlation is also observed between the diminished sensitivity in the middle frequency region of about 1000-3000 Hz in the listening tests and the diminished activity at the temporal lobes in the brain maps. Therefore listening tests can be used as reliable evidence to support the results of the Listening Therapy, as they are replicated by the QEEG data.
It is nowadays generally accepted in the medical society that music stimulates both the physical and psychological conditions of patients, as referred to in the Introduction of this paper.
In a recent publication of a German medical study [20] 60 subjects were randomly assigned to three groups that listened to various compositions by W. A. Mozart, J. Strauss Jr., or ABBA for 25 minutes. Their serum cortisol concentrations, heart rate, and blood pressure were measured before and after the listening sessions.
The same variables were measured in a control group of 60 subjects who did not listen to music but rested in silence. The data of the first group were found to have significant improvements as compared to the control groups and were most pronounced with Mozart music.
The present work illustrates that the Tomatis Listening Therapy, largely based on Mozart music, is even more effective and much more powerful than plainly listening to music.
Acknowledgements
The authors would like to thank all collaborators who contributed with their involvement in the Tomatis therapy. We particularly like to mention the staff of the Atlantis Institute and Mozart Brain Lab of Sint-Truiden, Belgium, for executing the therapy and gathering data over so many years. A special word of appreciation concerns Astrid Vervoort and Ann de Voigt for their personal and special support for so many years, with the therapy as well as with advice. Special thanks to the neurologists Dr. Van den Bergh and Dr. van Deun for guiding the QEEG measurements.
Declarations
The patients, with fictive names, or their representatives provided their written informed consent to use their data in this study.
- Tomatis AA (1963) l’Oreille et le Langage. Editions du Seuil, France. Also: The Ear and the Language. Moulin Publishing, Ontario, 1996. ISBN 0969707983.
- Sacks O (2007) Musicofilia, Tales of Music and the Brain. ISBN 9780330418379.
- Doidge N (2015) The Brain’s Way of Healing. Penguin Random House, UK. ISBN 9781846144240.
- Gerritsen J (2009) A review of research done on Tomatis auditory stimulation. www.listenwell.com and Developmental Disabilities 38: 567.
- Vervoort J, de Voigt MJA (2007) The improvement of severe psychomotor and neurological dysfunctions treated with the Tomatis Audio-Psycho-Phonology method as measured using EEG-brain-map and AEP. J Neurotherapy 11: 37-49.
- De Voigt Martien, Vervoort Jozef (2020) Listen to Live – our Brain and Music; the Tomatis Listening training and therapy. ISBN 9781782225843.
- Madaule P (1994) When listening comes alive. Moulin Publ., Ontario, ISBN 0969707916.
- Zastrow J (2015) Psychoacoustics from a medical point of view: similarities with ENT therapeutic practices. Proc. Int. congress on Audio-Psycho-Phonology-Evolved, 19-20 September 2015, Sint-Truiden, Belgium.
- Tomatis AA (1972) Education and Dyslexia (English), also Education et Dyslexie (French). E.S.F. In Coll. Sciences de l'Education: AIAPP Editions, Fribourg, France.
- Tomatis AA (1981) La Nuit Uterine: Verlag Editions Stock, Paris. See also: Der Klang des Lebens. Rowohlt Taschenbuch Verlag GMbH, Reinbeck. ISBN 3499187914.
- Tomatis AA (1989) Vers L’Ecoute Humaine. Tome 2, Zimmermann D (Ed) ESF, Paris, ISBN 2.7101.0751.1.
- Tomatis AA (1991) The conscious ear. Thompson, B.M. (Ed). Station Hill Press Inc, Barry town, New York 12507, ISBN 0882681087.
- Van den Bergh W (1998) Die Neurologischen Basis der Audio-Psycho-Phonologischen Therapie bei Sprachentwicklungsstörungen und Legasthenie. (The Neurological basis of the APF Therapy at Speech development and reading disorders). Vervoort J, Vervoort MJ (Eds) . Atlantis Instituut, Sint-Truiden, Belgium.
- Pinkerton F (1989) A neurophysiological study of children with reading, writing and spelling difficulties. Dev. Med. Chil. Neurol 31: 569-81.
- Mason MS, Mellor DH (1984) Middle latency and late cortical evoked potentials in children with speech and language disorders. Electroencephalogr. Clin Neurophysiol 59: 297-309.
- Tallal P (1996) Language comprehension in language-learning impaired children improved with acoustically modified speech. Science 271: 81-4.
- Merzenich MM (1996) Temporal processing deficits of language-learning impaired children ameliorated by training. Science 271: 77-81.
- Sollier P (2005) Listening for Wellness. The Mozart Centre Press, Walnut Creek, CA 94598, USA, ISBN 0-976363909.
- Tomatis AA (1991) Pourquoi Mozart (Why Mozart). Fixot, Paris France, ISBN 9782876-451070.
- Trappe H.J. & Voit G (2016) The Cardiovascular Effect of Musical Genres – A randomized controlled study on the effect of compositions by Mozart, Strauss and ABBA. Dtsch Arztebl Int 113: 347–52.
FIGURE 1
*The blue curve represents the air conduction and the red one the bone conduction. Intermediate frequencies at 750, 1500, 3000 and 6000 Hz are omitted for clarity [5,6]
Figure 1: The listening test with ideal curve, constructed by Tomatis
FIGURE 2
*The air conduction is represented in blue and the bone conduction in red, both for the right (R) and left ear (L). The little red vertical dashes bottom indicates localization (spatiality) errors. The auditory laterality is measured at the 5 frequencies indicated; V means front (sensitive right) an H behind (sensitive left). There is some change in the laterality from left to right during the therapy.
Figure 2: Erhardta�s listening tests before, 2005 (above), and after the therapy, 2008 (below) [6]
FIGURE 3
*The data were taken with the eyes closed (odd-ball paradigm) and passive condition with 80 dB binaural tones. A clear N100 response is present, but no clear N200 nor P300 response
Figure 3: Cognitive auditory evoked potentials following the Erhardt�s rare tones before therapy in 2005 [6]
FIGURE 4
*The vertical color bars indicate the activity in �V. There is abnormally strong d activity frontal and in the � map the damaged lesion area is seen left temporal. Moreover, the a activity is asymmetric
Figure 4: Erhardt�s brain map before the therapy, with d top left, ? bottom left, a top right and � bottom right [6]
FIGURE 5
.jpg)
.jpg)
*Left, right and front (below) views, with the subject left, the control data in the middle and the difference between them on the right. The d activity is plotted at the top, below it the ? activity, the a activity and the � activity at the bottom. The maximum Z-scores or standard deviation, given in �V squared, are indicated by Max / Min in each left upper corner
Figure 5: Erhardt�s brain map with the eyes closed, after the therapy [6]
FIGURE 6
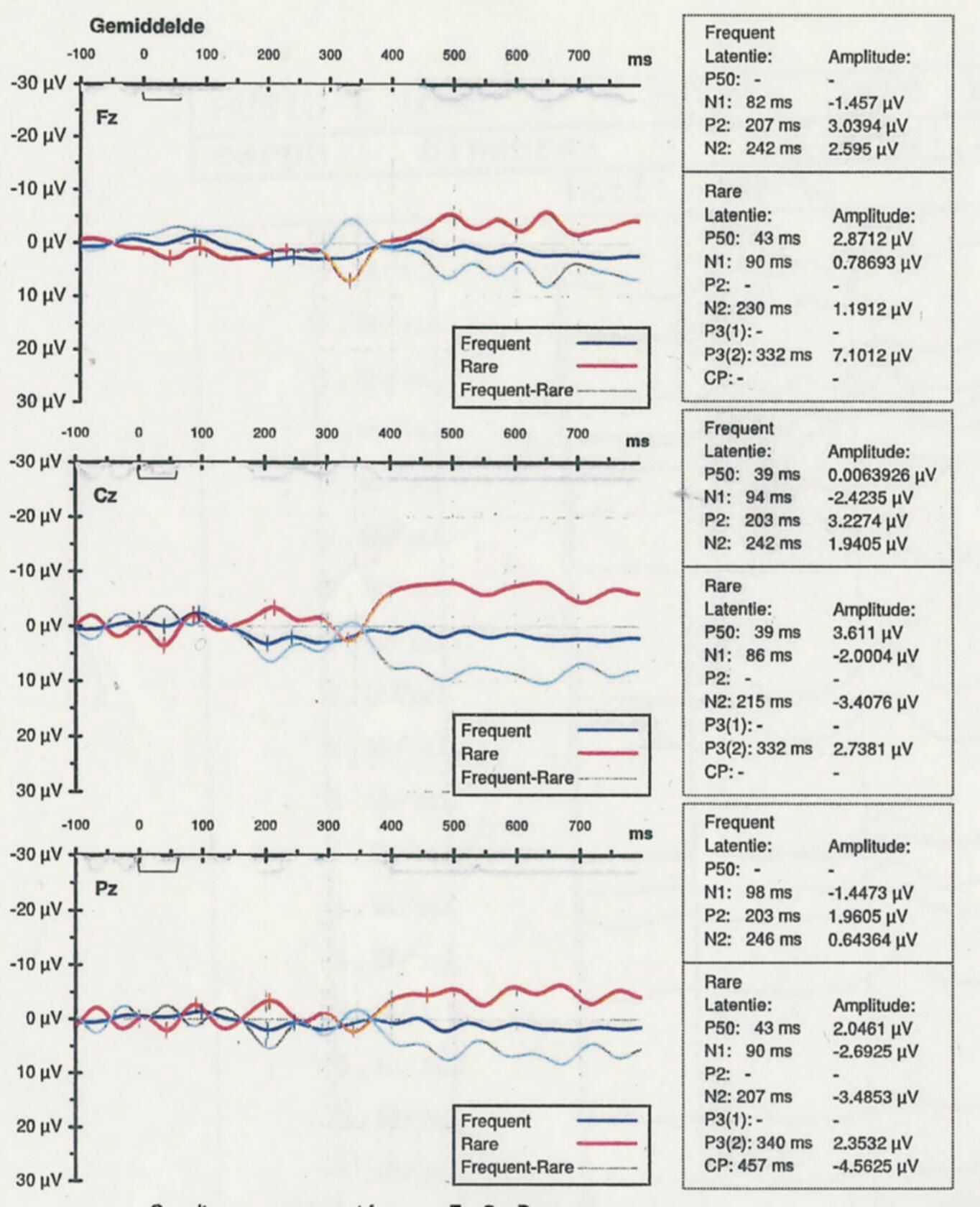
*Note that the negative potentials are plotted upwards. Most of the AEP�s are present, particularly the attention potential P300(2) with the rare tones (red curves) at 332 and 340 ms.
Figure 6: Part of Erhardt�s QEEG Cognitive Auditory Evoked Potentials, at Fz, Cz, and Pz, after the therapy in 2008, [6]
FIGURE 7
.JPG)
.JPG)
*See Figure 8 for the associated brain maps. The blue stars indicate left-right spatial errors in the air conduction, which disappear with stronger sound volume and the red crosses indicate those in the bone conduction
Figure 7: Listening tests before (above) and after a large part of the therapy (below) of an autistic little boy [5,6]
FIGURE 8
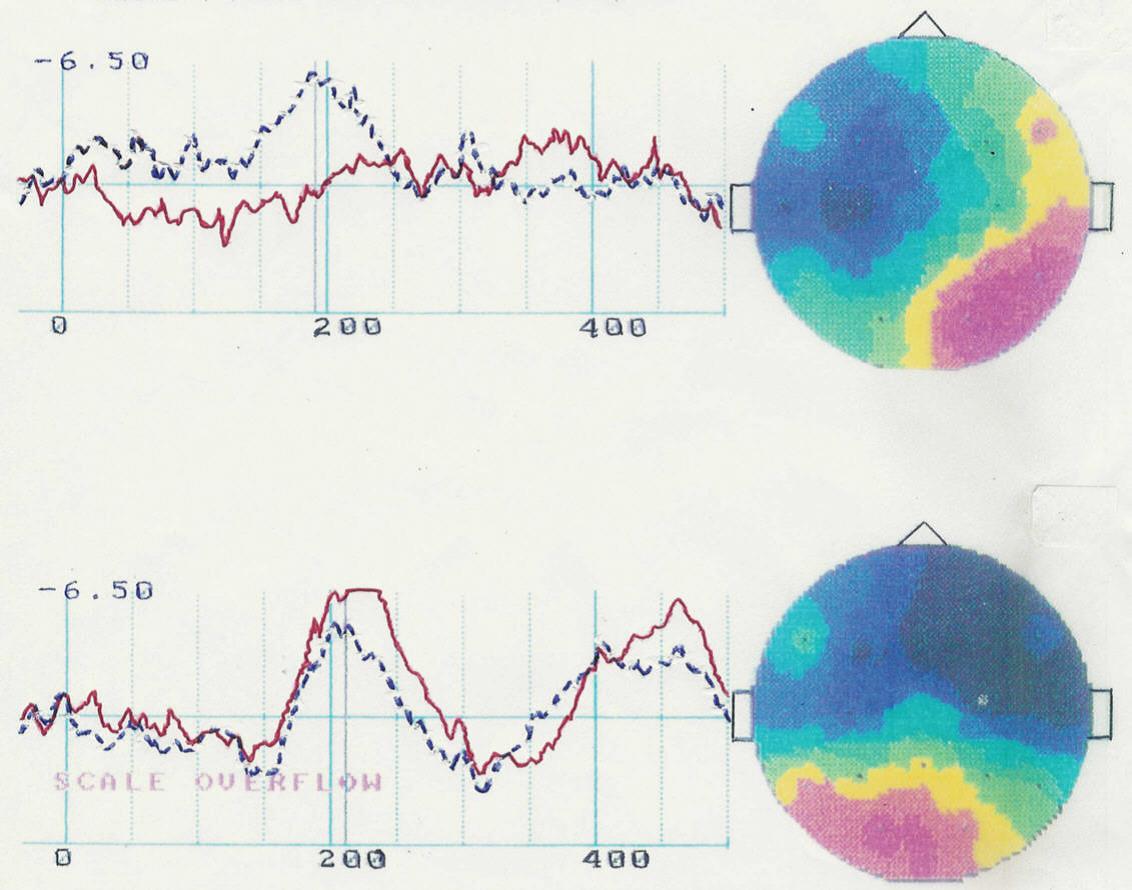
*The solid red line represents the T4 complex and the broken blue one the T3 complex. The T complexes are measured as a sum of the P100, N100, P200, and N200 intensities. Normally T4=T3 when language disorders are absent, which is only the case after the therapy. Note that in the brain map the blue color represents electrical negative voltage, i.e. high brain activity and the red color therefore low brain activity. After the therapy the brain activity left-right is much more harmonized.
Figure 8: Middle latency auditory evoked potentials (MLAEP�s) and d brain maps of Freddy before (above) and after the therapy (below) [5,6]
FIGURE 9
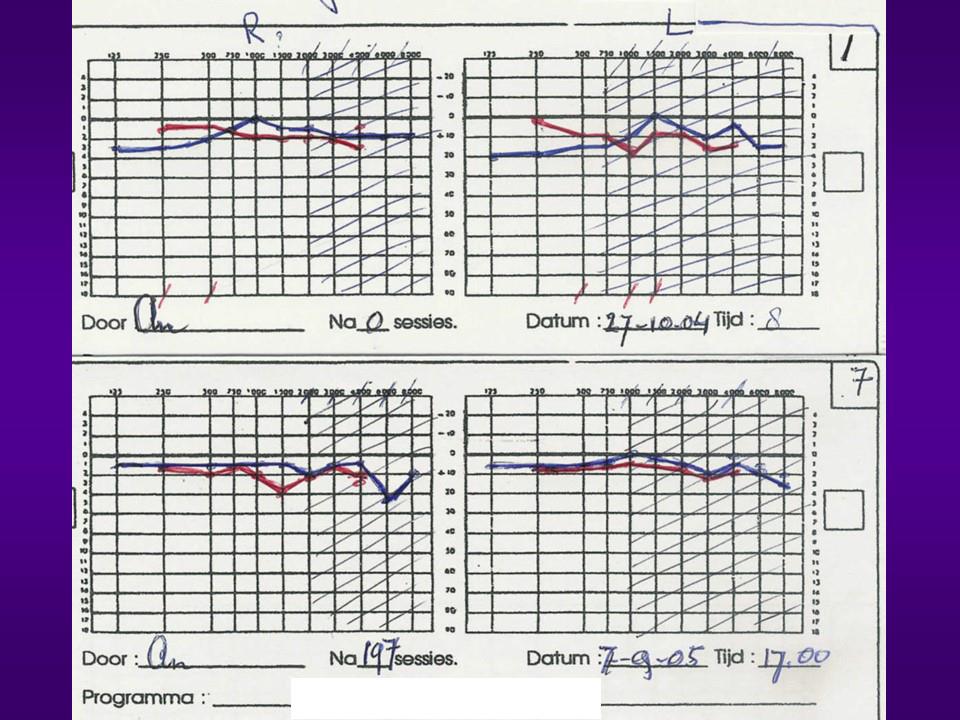
Figure 9: Listening test of Maurits before (above) and after (below) part of the therapy [6]
FIGURE 10
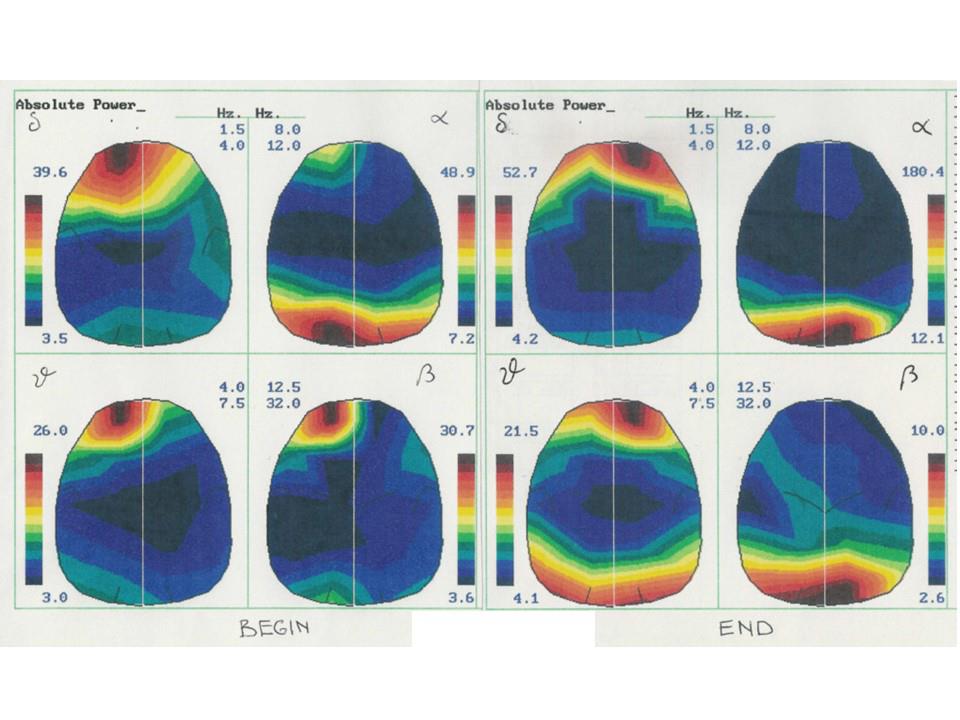
*Note the scales in �V, on the sides, which indicated much stronger a and weaker � strengths after the therapy
Figure 10: Brain maps of Maurits before (left) and after (right) part of the therapy [6]
FIGURE 11
Figure 11: AEP curves of Maurits before (left) and after (right) a large part of the therapy [6]
FIGURE 12
.jpg)
.jpg)
*The selectivity could not be measured and the auditory laterality is indicated at the bottom with V (front, sensitive right) or H (back, sensitive left)
Figure 12: The first listening test of Nike in 2016 (above) and after three years (below)
FIGURE 13
Figure 13: Brain maps of Nike before (October 2016, left) and after (August 2019, right) the therapy, taken with the eyes open. The Z-scores are indicated in upper left corners
FIGURE 14
*The red curves are taken with attention to the rare tones (given at 1500 Hz) and the blue ones as reactions to the same repeated tones of 1000 Hz. Note that positive potentials are plotted downwards. The blue areas indicate the possible location of the important P300 potential
Figure 14: Measured AEP�s of Nike before (left) and after (right) the therapy for the three positions on the skull Fz, Cz, Pz
FIGURE 15
.jpg)
.jpg)
Figure 15: First listening test of Rick (above) at age 7 yrs. and already after ~3 months and first cycles of listening (below). The selectivity could not be tested, therefore assumed closed, and the laterality is indicated at the bottom with L left, R and V right. Spatiality errors are indicated with red dashes at the bottom
FIGURE 16
.jpg)
.jpg)
Figure 16: Brain maps of Rick, with the eyes open, at age 7 yrs. (left) and after ~3 months (right)
FIGURE 17
Figure 17: AEP�s measured of Rick with the same setup as the brain maps, at age 7 yrs. (left) and after ~3 months (right). The blue areas indicate the possible location of the P300 potential
Figures at a glance