Effectiveness and Quality of Life After Elective Unilateral Uterine Artery Embolization in Women with Symptomatic Unilateral Located Fibroids
Received Date: February 10, 2025 Accepted Date: March 10, 2025 Published Date: March 13, 2025
doi:10.17303/jfsrh.2025.2.101
Citation: Sven-Ole Adriaansens MD, Alexander Venmans MD PhD, Paul Lodder PhD, Rozemarijn de Kruijk MD, Ekin Öztürk MD, et al. (2025) Effectiveness and Quality of Life After Elective Unilateral Uterine Artery Embolization in Women with Symptomatic Unilateral Located Fibroids. J Fertil Steril Reprod Health 2: 1-10
Abstract
Purpose: To determine the effectiveness and quality of life of elective unilateral uterine artery embolization (uUAE) in selected women with symptomatic unilateral fibroids.
Methods: From a total of patients who underwent standard bilateral UAE (bUAE) between 2003 and 2018, a subset of patients who underwent unilateral (uUAE) was analyzed. The inclusion criteria were: 1) symptomatic uterine fibroids, 2) presence of unilateral fibroids confirmed by MRI, 3) intentional unilateral embolization. Imaging and clinical results three months after uUAE were compared with baseline imaging and clinical results. Primary objective was to assess the clinical outcome using the questionnaire Uterine-Fibroid Symptom and Quality of Life (UFS-QOL) at baseline and 3 months follow-up. Secondary objectives were to assess the degree of fibroid infarction, change of fibroid and uterine volume using MR imaging.
Results: From a total of 1,588 patients, the study group included 34 patients with symptomatic unilateral fibroids who underwent an intentional uUAE. Baseline mean fibroid volume was 281.3cc (median 180.4cc, range 9.1–1059cc). After uUAE at median 3 months follow-up the mean fibroid volume was 145.7cc (median 68.5cc, range 4.4–1013cc); a significant fibroid volume reduction (p<0.0001). Comparing the median 3 months follow-up HR-QOL total score to baseline demonstrated a significant improvement of quality of life with a score difference of 29.6 (6.6, 52.5; 95% CI) points, respectively 39.3 (27.9 SD) vs. 19.5 (18.5 SD) points (lower scores indicate better quality of life). There were no complications.
Conclusion: Elective unilateral embolisation in carefully selected patients with symptomatic unilateral localized uterine fibroids is safe and effective and yields a high rate of fibroid infarction as the basis for an expected sustained decrease in symptoms, improvement in quality of life and patient satisfaction.
Keywords: Unilateral Uterine Artery Embolization; Unilateral Embolization; Uterine Atery Embolization; Uterine Fibroids; Gynecology
Introduction
Uterine atery embolisation (UAE) is a worldwide accepted endovascular treatment option for women with symptomatic uterine fibroids [1,2]. With the introduction in 1995 of UAE as a stand-alone treatment for symptomatic uterine leiomyomatosis, the adage is that embolization must be bilateral with occlusion of both uterine artery branches to the perifibroid plexus, since both left and right uterine arteries have cross-linked uterine collaterals. [3]. Standard bilateral UAE (bUAE) is essential for complete fibroid infarction leading to a successful clinical outcome. Performing unilateral (single-side) uterine artery embolization offers no complete infarction due to persistent perfusion through collaterals from the opposite site. This concept is supported by published work of clinical failure after unilateral UAE (uUAE) [4-6]. However, predominantly unilateral feeding of fibroids was found to occur in 36.5% of cases [7]. In these cases, uUAE would be sufficient in achieving complete fibroid infarction. This may offer benefits for the patients through reduced risk of ovarian- and endometrial damage and is of interest to young fertile women with a desire for children or older women who do not want to be at risk for premature menopause. Moreover, uUAE causes less postprocedural pain due to reduction of uterine myometrial ischaemia [8]. The purpose of this study is to evaluate the effectiveness and quality of life after uUAE in symptomatic women with unilateral located uterine fibroids.
Methods
Patients
In this single-center (Elisabeth Tweesteden Hospital Tilburg, The Netherlands) retrospective study with prospectively collected data. From a total of patients who underwent standard bilateral UAE (bUAE) between 2003 and 2018, a subset of patients who underwent unilateral (uUAE) was analyzed. This subset of patients was collected through a retrospective digital search in the PACS system reports, using "unilateraal, eenzijdig, eenzijdige, unilaterale, myoom, embolisatie" Dutch keywords on all 1.588 fibroid embolisation reports throughout the period 2003-2018.
The final inclusion criterium was the triade: 1) patient with symptomatic unilateral uterine fibroid disease on MR, 2) unilateral vascular supply by the ipsilateral uterine artery seen with angiography, and 3) followed by a unilateral UAE. In this subgroup of women clinical outcomes (UFS-QOL questionnaire, with 6 subscales; symptom severity score, concerns, activities, energy, mood, control, self-conscious and sexual function) and MRI images (fibroid infarction, uterine- and fibroid volume reduction) three months after uUAE were compared with baseline data.
The study was approved by the local institutional review board and medical ethics committee. The study was conducted in accordance with the Health Insurance Portability and Accountability Act and the principles of the Declaration of Helsinki. Informed consent is not required at our institution for retrospective studies of this type.
The uUAE group was defined as women with an elective embolization of one single uterine artery with unilateral fibroids confirmed by MRI and angiography, with a contralateral uterine artery supplying normal myometrium.
The inclusion criteria for participation in the study were: 1) patients with symptomatic uterine fibroids such as heavy menstrual bleeding, pelvic pain and/or bulk-related symptoms, 2) presence of unilateral fibroids confirmed by MRI, and 3) intentional unilateral embolization.
The exclusion criteria were 1) technical failure to catheterize both uterine arteries, 2) absence of a uterine artery, 3) supply from a hypertrophied ovarian artery to the fibroid, 4) additional uterine pathology (such as adenomyosis, malignancy, or otherwise), and 5) a history of UAE.
Measures
In this retrospective study with prospective collected data, outcome measures were retrieved through chart review. The imaging and clinical results three months after uUAE were compared with the baseline imaging and clinical results.
Health-related Quality of Life
To determine the effectiveness and quality of life of uUAE for symptomatic unilateral fibroid disease, the primary objective was to assess the clinical outcome using the questionnaire Uterine-Fibroid Symptom and Quality of Life (UFS-QOL) at baseline and at 3 months after the intervention. The questionnaire asks patients to respond to 37 questions measuring the extent to which their uterine fibroid has affected their quality of life. An example item is “During the previous 3 months, how often have your symptoms related to uterine fibrosis interfered with your physical activities?”. Participants can respond on a scale of 1 (“None of the time”) to 5 (“All of the time”). This questionnaire is validated and standardized containing the health-related quality of life (HRQOL) and symptom severity score (SSS) [9].
Fibroid Characteristics
The secondary objectives were to assess the degree of infarction of the uterine fibroid, change of fibroid and uterine volume using T2, T1 and contrast-enhanced MRI images at baseline and at 3 months after UAE.
The uterine fibroid volume was calculated using the ellipsoid formula: length x width x height x 0.5233 [10]. Two experienced radiologists (AV, PL) assessed the fibroid infarction rate by using the same volumetric measurement and infarction rates were categorized in 4 infarction rate groups, i.e. infarction rate group 100%, 90-99%, 50-89% and <50% similar to the study method of Stall et al. [11]. The pre- and post-procedural MRI images were analyzed according to uterine- and fibroid volume, fibroid number and location. Fibroid expulsion was classified as 100% infarction. Complications were obtained from the hospital records, the interventional radiology clinic chart or by patient self-report.
Menopause Symptoms
During follow-up women were asked if they experienced symptoms related to transient or permanent premature menopause potentially caused by non-targeted embolization to the ovaries through angiographically apparent or hidden uterine-ovarian shunts.
Satisfaction with Intervention
Three months after the intervention, all patients were asked to what extent they were satisfied with the results of the intervention. Choice answers; very satisfied, satisfied, neutral and don't know yet.
Procedure
All participants underwent uUAE, at the side of the location of the unilateral fibroid disease. All procedures were executed by three experienced interventional radiologists (AV, PL). Patients received a ‘patient-controlled analgesia’ (PCA) pump (Dompiridol and Dipidolor), 5-10 mg Diazepam p.o., 1000 mg Paracetamol p.o. and 1x500 mg Naproxen, 30 minutes before the intervention.
The puncture side of the common femoral artery was numbed with local anaesthetic (lidocaine 1%). The access to the femoral arteries was obtained bilaterally followed by positioning a 4F C2-catheter in the contralateral internal iliac artery. Digital subtraction angiography (DSA) was performed to identify the uterine artery and its branches. In case the 4 Fr C2 catheter blocked the uterine artery impairing normal blood flow, a microcatheter was used. Microcatheter sets consisted of a Y-connector, an Embocath microcatheter (Merit Medical Systems; Utah, USA) and 0.014 inch microwire Transend (Stryker Neurovascular; Fremont, USA). Omnipaque 300 mg I/ml contrast medium was used to achieve angiographic images with two frames per second. After selective catheter placement three DSA runs were performed, i.e. from each side separately and both sides together. The obtained angiographic images were per-procedural evaluated to identify the afferent blood supply and enhancement of the fibroid. Along with the angiographic findings and the baseline MR images the interventionalist decided to continu the intervention by performing a selective uUAE procedure from the right or left uterine artery.
Different types of embolic material were used depending on the preference of the interventional radiologist; EmbozeneTM microsphere ranging in size between 500-900μm (Varian Medical Systems, Palo Alto, CA, USA); Embosphere® microsphere sizes between 500-1300μm (Merit Medical Systems; Biosphere Medical, Roissy, France); HydropearlTM microspheres 600-1100±75μm (Terumo; MicroVention, Saint-Germain-en-Laye, France) and SpongostanTM gelatin sponge (Ethicon, Johnson & Johnson Medical N.V.). The angiographic embolization end point was defined when complete stasis in the distal part of the uterine artery was obtained with DSA confirmation also after 5 minutes of waiting. After each uUAE procedure an additional separate DSA of the contralateral uterine artery was performed to assure 1) free of intratarterial contrast flow through a patent contralateral uterine artery and its branches toward the uterine stroma, and 2) no contrast perfusion from its side to the fibroid.
After the intervention the groin sheaths were removed and manual pressure was put on both the puncture sides for at least ten minutes and no closure devices were used. After the procedure patients were transferred to the recovery unit. Postoperative care consisted of 6 hours of bedrest and adequate pain control. Pain medication included 1000 mg paracetamol supp. 4/day, 500mg Naproxen supp. 2/day and all patients were instructed how to use the PCA-pump.
Statistics
Descriptive statistics for continuous variables were expressed in terms of mean, standard deviation, median and range. Categorical variables were described in terms of frequencies and percentages.
For the UFS-QOL, subscale scores were calculated by summing all items measuring a subscale construct and transforming the resulting score to a scale ranging from 0 to 100. Subscale scores of patients who did not respond to more than half of the subscale items were considered missing on that particular measurement occasion. The item scores on the questionnaire on satisfaction rate after uUAE were summed to obtain a total satisfaction score for each participant.
The difference between baseline and 3-month post embolization was expressed in terms of means and 95% confidence intervals. Paired t-tests were used to test the null hypotheses that these differences between baseline and 3-months were equal to zero in the population. Statistical significance was concluded in the p-value was lower than the significance level of 0.05.
All analyses were conducted using the software R-studio (version 4.1.1).
Results
From a total of 1,588 patients who underwent UAE between 2003-2018 the following patients were excluded for the following reasons: bilateral embolisation (n=1.531). Of the remaining 57 patients the following patients were excluded for the following reasons; previous UAE (n= 4), ovarian supply to the fibroid (n=2), accompanying adenomyosis (n=3), sarcoma (n=1), persisted post-partum bleeding (n=1) and a unilaterally localized fibroid treated (erroneously) unilaterally while bilaterally fed visible on angiographic examination (n=12).
The final study group included 34 patients with symptomatic unilateral uterine fibroids who underwent an intentional uUAE. All 34 patients underwent pre- and post-procedural imaging. At baseline the mean fibroid volume was 281.3cc (median 180.4cc, range 9.1–1059cc). After uUAE at median 3 months follow-up the mean fibroid volume was 145.7cc (median 68.5cc, range 4.4–1013cc) resulting in a significant fibroid volume reduction (p<0.0001) (Table 1).
Figure 1 demonstrates graphically the individual steep decrease and mean steep decrease in fibroid volume comparing the fibroid volume at baseline with 3 months after uUAE. The degree of fibroid infarction after intentional uUAE in 34 patients was 100% in 25 patients, 90-99% in 3, 50-89% fibroid infarction in 3 and less than 50% in 3 patients (Figure 2).
All 34 patients completed the questionnaires pre-procedural and the questionnaires at three months after the intervention
The median baseline score for total HR-QOL was 39.3 points (27.9 SD). Comparing the median 3 months follow-up HR-QOL total score to baseline demonstrated a significant improvement of quality of life with a score difference of 29.6 (6.6, 52.5; 95% CI) points, respectively 39.3 (27.9 SD) vs. 19.5 (18.5 SD) points (lower scores indicate better quality of life). Table 2 demonstrates improvement of all 6 UFS-QOL subscales.
There were no complications obtained from the hospital records, the interventional radiology clinic chart or by patient self-report. There were no clinical signs or women suffering from symptoms related to transient or permanent premature menopause caused by ovarian damage. Three months after the intervention 75% of patients were satisfied or very satisfied, 19% neutral and 6 % don’t know yet.
Discussion
This retrospective study demonstrated the efficacy and safety of uUAE in a selected subgroup of women with unilateral uterine fibroid disease. The results are based on clinical and imaging outcomes (respectively UFS-QOL and MR imaging). In this cohort of patients treated with uUAE more than 80% of patients showed an infarction rate of nearly 100%, with significant fibroid volume reduction at 3 months follow-up, significant improvement of HR-QOL and patient’s satisfaction. Regarding the safety aspect with uUAE, the results also do not indicate an increase in minor or major complications compared to bUAE.
In the literature, the reported study on uUAE reported 48 patients of whom 30 underwent intentional uUAE versus uUAE due to technical failure caused by anatomical constraints [12]. The clinical response with a reduction in menorrhagia at 1 year follow up was seen in 86% of those with a dominant arterial supply to the fibroids. There was a similar improvement in dysmenorrhea and bulk-related symptoms in 86% and 76% respectively at 1 year. Of those patient undergoing MRI, the fibroid infarction rate was 83%. Uterine/dominant fibroid volume reduction was 49% at mean 9.8 months. The overall conclusion was that elective uUAE can achieve positive long-term clinical outcomes in patients with dominant unilateral arterial supply to fibroids.
A second retrospective comparative study regarding elective uUAE of 28 patients with uterine myomatosis showed similar results to bilateral embolization [11]. No significant differences were seen regarding the percentage of fibroid infarction (uUAE with 92% vs. bUAE 88%), which is a known factor for long-term clinical outcomes and patient satisfaction [13]. Using the chief symptom resolution score as well as the satisfaction score, both groups showed no statistical differences at 3 months follow-up (clinical outcome 2.1 vs. 1.9; P=27 and satisfaction score 4.0 versus 4.0; P=.72). Follow-up volume reductions were not reported.
The third retrospective study of uUAE for fibroids in 26 patients showed an overall clinical success rate of 88% at 6 months follow-up, stating that elective uUAE is an appropriate treatment in patients with a dominant uterine artery [14]. Patients were asked to express the level of satisfaction on a five-point scale. Fifteen patients (58%) were very satisfied, seven (27%) were satisfied. Four patients (15%) were dissatisfied with the clinical results. The degree of infarction and uterine/fibroid volume reduction after uUAE were not mentioned.
Unlike the three previous studies, we used the standardized HR-QOL questionnaire scoring for 6 UFS-QOL subscales [9]. Our study demonstrated significant improvement of quality of life with a score difference of 29.6 (6.6, 52.5; 95% CI) points, respectively 39.3 (27.9 SD) at baseline vs. 19.5 (18.5 SD) points at 3 months follow-up (lower scores indicate better quality of life). All standardized 6 UFS-QOL subscales showed improvement at 3 months follow-up after uUAE. Our home-made questionnaire on satisfaction rate after uUAE presented 75% (very)satisfied patients at 3 months follow-up. Our study matches the observations of the authors mentioned above also with regard to the infarction rate of 80% of patients with nearly 100% of fibroid infarction, and a significant fibroid volume reduction 53% (145.7cc at baseline; median 68.5cc at 3 months follow-up, p<0.0001).
Despite the fact that different measurement methodologies were used in this and the previously mentioned studies, we believe we may conclude that over-all a significant symptom improvement and degree of patient satisfaction was seen after uUAE in a preselected patient population with unilaterally localized symptomatic uterine fibroids. Likewise, in all studies listed, the vast majority showed a high fibroid infarction rate of 80% or more after uUAE in this selected subgroup of patients.
Moreover published data regarding uUAE in women with symptomatic uterine fibroids mention several advantages, such as reduced fluoroscopy time, reduced use of contrast, reduced post-procedural pain, probably decreased risk by ½ of non-targeted embolization to the endometrium and ovary with potentially better pregnancy outcome in young women and less risk of transient/permanent premature menopause in older women [11]. The uUAE approach may be of particular interest to young women who want to become pregnant and/or women with fertility issues, as a “fertility-sparing technique” [15, 16]. The benefit of uUAE may perhaps also apply to older patients, who want to minimize the risk of premature menopause followed by early osteoporosis, moodswings, and other post-menopausal symptoms.
This study of elective uUAE for unilateral fibroids has several limitations that require further research to determine its applicability and long-term efficacy. Although the data were prospectively collected, the retrospective design of the study and the relatively small number of patients with short-term outcomes limit the validity of the data. Second, the absence of a control group treated with bUAE can be seen as a potential disadvantage. Whether the unilateral approach causes less damage to the endometrium and ovary, and truly results in more successful pregnancies and reduced risk of premature menopause, remains to be seen in future studies with larger numbers of patients and longer follow-up.
Conclusion
Elective unilateral embolisation in carefully selected patients with symptomatic unilateral localized uterine fibroids is safe and effective and yields a high rate of fibroid infarction as the basis for an expected sustained decrease in symptoms, improvement in quality of life and patient satisfaction.
- Keung JJ, Spies JB, Caridi TM (2018) Uterine artery embolization: A review of current concepts. Best Practice & Research: Clinical Obstetrics & Gynaecology, 46: 66-73.
- ACOG practice bulletin (2008) Alternatives to hysterectomy in the management of leiomyomas. American College of Obstetricians and Gynecologists. Obstet Gynecol. 112: 387-400.
- JH Ravina, D Herbreteau, N Ciraru-Vigneron, et al. (1995) Arterial embolisation to treat uterine myomata. Lancet, 346: 671-2.
- McLucas B, Reed RA, Goodwin S, et al. (2002) Outcomes following unilateral uterine artery embolisation. Br J Radiol. 75: 122-6.
- K Gabriel-Cox, GF Jacobson, MA Armstrong, YY Hung, LA Learman (2007) Predictors of hysterectomy after uterine artery embolization for leiomyoma. Am J Obstet Gynecol. 196: 588.e1-6.
- JB Spies, ER Myers, R Worthington-Kirsch, et al. (2005) The FIBROID Registry: symptom and quality-of-life status 1 year after therapy. Obstet Gynecol. 106: 1309-18.
- Chen CL, Xu YJ, Liu P, et al. (2013) Characteristics of vascular supply to uterine leiomyoma: An analysis of digital subtraction angiography imaging in 518 cases. Eur Radiol. 23: 774-9.
- Aziz A, Petucco OM, Makinoda S, et al. (1998) Transarterial embolization of the uterine arteries:patient reactions and effects on uterine vasculature. Acta Obstet Gynecol Scan, 77: 334-40.
- Spies JB, Coyne K, Guaou Guaou N, Boyle D, Skyrnarz-Murphy K, Gonzalves SM (2002) The UFS-QOL, a new disease-specific symptom and health-related quality of life questionnaire for leiomyomata. Obstet Gynecol. 99: 290-300.
- Siskin GP, Beck A, Schuster M, Mandato K, Englander M, Herr A (2008) Leiomyoma infarction after uterine artery embolization: A prospective randomized study comparing tris-acryl gelatin microspheres versus polyvinyl alcohol microspheres. J Vasc Interv Radiol. 19: 58-65.
- Stall L, Lee J, McCullough M, Nsrouli-Maktabi H, Spies JB (2011) Effectiveness of elective unilateral uterine artery embolization: A case-control study. J Vasc Interv Radiol. 22: 716-722.
- Bratby MJ, Hussain FF, Walker WJ (2008) Outcomes after unilateral uterine artery embolization: A retrospective review. Cardiovasc Intervent Radiol. 31: 254-9.
- Pelage JP, Guaou NG, Jha RC, Ascher SM, Spies JB (2004) Uterine fibroid tumors: Long-term MR imaging outcome after embolization. Radiology, 230: 803-9.
- K Pyra, M Szmygin, H Szmygin, S Woźniak, T Jargiełło (2022) Unilateral Uterine Artery Embolization as a Treatment for Patients with Symptomatic Fibroids-Experience in a Case Series Medicina (Kaunas) 58: 1732.
- JM Pisco, M Duarte, T Bilhim, et al. (2017) Spontaneous Pregnancy with a Live Birth after Conventional and Partial Uterine Fibroid Embolization. Radiology, 285: 302-10.
- O Serres-Cousine, FM Kuijper, E Curis, D Atashroo (2021) Clinical investigation of fertility after uterine artery embolization. Am J Obstet Gynecol. 225: 403.e1-403.e22.
FIGURE 1
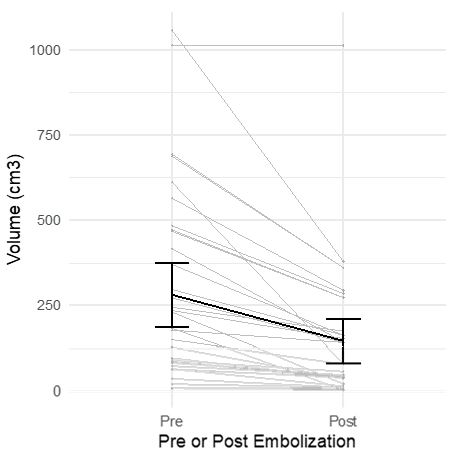
Figure 1: Individual change (grey) and mean change (black) in fibroid volume before and after embolization
FIGURE 2
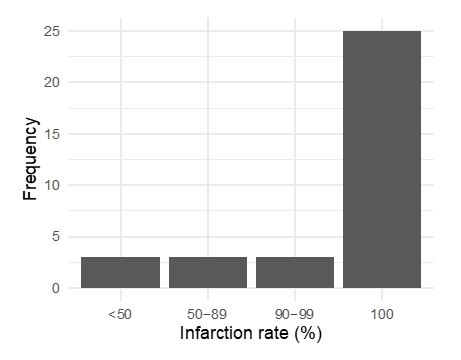
Figure 2: Number of patients with particular infarction rate (N=34, Median = 100, Interquartile range = 50 to 100)
Tables at a glance
Figures at a glance