Nasal Complement Procedures Performed Through the Le Fort I Approach: A Practical Technical Note
Received Date: December 31, 2025 Accepted Date: January 07, 2026 Published Date: January 10, 2026
doi: 10.17303/jdoh.2026.13.101
Citation: Bruno Nifossi Prado, Raphael Capelli Guerra, Bianca Pulino, Lucas Cavalieri (2026) Nasal Complement Procedures Performed Through the Le Fort I Approach: A Practical Technical Note. 13: 1-5.
Abstract
This technical note describes practical nasal complementary procedures that can be safely incorporated into Le Fort I osteotomy. Septal resuturing, limited septoplasty, inferior turbinate reduction, nasal tip grafting, and nasal dorsum shaping can be performed through the same surgical field with minimal added operative time. These maneuvers help prevent postoperative nasal airway obstruction, enhance nasal aesthetics, and reduce the need for secondary rhinoplasty. Their clinical relevance aligns with the functional and aesthetic expectations of modern orthognathic surgery.
Keywords: Orthognathic Surgery; Le Fort I Osteotomy; Nasal Septum; Turbinectomy; Nasal Tip Graft; Rhinoplasty; Airway Obstruction.
Introduction
Patient Selection and Indications for Adjunctive Nasal Procedures
Adjunctive nasal procedures were selected based on preoperative clinical examination, facial analysis, and intraoperative findings. Septoplasty was indicated in patients presenting with clinically significant septal deviation associated with nasal airway obstruction. Inferior turbinate reduction was performed in cases of turbinate hypertrophy contributing to impaired nasal airflow. Nasal tip grafting was considered when maxillary repositioning resulted in reduced nasal tip support, tip ptosis, or altered nasolabial angle. Dorsal shaping was indicated for patients presenting with preexisting or surgery-related dorsum irregularities or asymmetries. The alar cinch suture was routinely employed to prevent postoperative widening of the alar base following maxillary advancement or impaction (Table 1).
Nasal Septum Resuturing and Limited Septoplasty
During maxillary down-fracture, the nasal septum becomes fully detached from its maxillary articulation, requiring stabilization to prevent deviation and obstruction [1, 4]. After maxillary repositioning, the septum is sutured to the anterior nasal spine using 2-0 nylon sutures.In cases of maxillary impaction or transverse/asymmetric repositioning, limited septoplasty is performed by trimming the cartilaginous septum to prevent postoperative deviation [2, 4].
Inferior Turbinate Reduction
Maxillary intrusion or posterior repositioning may reduce intranasal space, causing inferior turbinate impingement [3, 7]. After down-fracture, the inferior turbinates are directly visible; partial turbinectomy is performed using electrocautery to reduce turbinate bulk and minimize postoperative airway obstruction (Figure 1).
This approach is particularly indicated in patients with turbinate hypertrophy or obstructive sleep apnea [7, 8].
Nasal Tip Grafting
Cartilage harvested from the septum can be used as a nasal tip graft, enhancing projection and definition without the need for external rhinoplasty incisions [5].A submucosal tunnel is created, the graft is inserted into the nasal tip region, and fixation is achieved with 5-0 nylon sutures (Figure 2).
Nasal Dorsum Shaping
Minor dorsal hump refinement is performed through an intranasal approach using manual rasping, allowing aesthetic improvement without requiring changes in the intubation route or extending operative time [6, 9, 10].
Alar Base Closure (Alar Cinch Suture)
Following maxillary repositioning, the alar base tends to widen due to the detachment of perinasal musculature and soft-tissue tension changes commonly observed after Le Fort I osteotomy. To prevent postoperative alar flaring and loss of nasal definition, an alar cinch suture is performed.
A transnasal 3–0 or 4–0 non-resorbable suture is passed through the fibro-muscular tissue of both alar bases, securing them centrally to maintain preoperative nasal width. This maneuver restores the natural tension of the nasolabial complex and prevents undesirable lateral displacement of the alar bases, which is frequently reported in maxillary advancement procedures [11, 12].The suture is tightened gradually to match the preoperative interalar distance and is fixed to the anterior nasal spine or soft-tissue midline.
This step adds minimal time to the procedure and provides reliable control of the nasal base, complementing other nasal refinements achieved during orthognathic surgery (Figure 3).
Postoperative Considerations
Early postoperative follow-up demonstrated subjective improvement in nasal airway patency and overall patient satisfaction in most cases. No major complications related to the adjunctive nasal procedures were observed. Mild nasal edema and transient congestion were common in the immediate postoperative period and resolved spontaneously. Given the technical nature of this report, quantitative functional assessments were not performed. Future prospective studies are warranted to objectively evaluate airway function and patient-reported outcomes following combined orthognathic and nasal procedures.
Discussion
Nasal anatomical changes are inherent to Le Fort I osteotomy, and associated nasal procedures are increasingly recognized as beneficiais [1, 3, 6]. Septal stabilization prevents deviation after maxillary repositioning, a complication well described in the literature [4].Inferior turbinate reduction improves nasal patency when maxillary movements reduce intranasal space [7, 8].Additionally, minor nasal aesthetic refinements—tip grafting and dorsal reshaping—enhance facial harmony and reduce the need for future rhinoplasty [5, 6, 9].These maneuvers add minimal surgical time, are performed through the same field, and can significantly improve postoperative satisfaction.
Although the present manuscript focuses on the technical description of adjunctive nasal procedures performed through the Le Fort I approach, it has some limitations. This technical note does not include quantitative postoperative assessments of nasal airway function, patient satisfaction scores, or objective airflow measurements. The absence of quantitative data reflects the primary objective of this report, which is to describe surgical techniques and intraoperative strategies rather than to evaluate clinical outcomes. Future prospective studies incorporating objective functional measurements and validated patient-reported outcome instruments are warranted to further assess the clinical efficacy of combining these procedures.
Nasal complement procedures performed during Le Fort I osteotomy are practical, efficient, and beneficial. Their integration into orthognathic surgery provides improved airway function, greater aesthetic refinement, and reduces the likelihood of future isolated nasal procedures.
- Weiss RO, Ong AA, Reddy LV, Bahmanyar S, Vincent AG, et al. (2021) Orthognathic surgery–Le Fort I osteotomy. Facial Plast Surg. 37: 703-8.
- Posnick JC, Agnihotri N, Managing (2011) chronic nasal airway obstruction at the time of orthognathic surgery: a twofer. J Oral Maxillofac Surg. 69: 5-701.
- Alande C, Vandersteen C, Masson Regnault E. Ostéotomie de Lefort, et al. (2022) obstruction nasale. Orthod Fr. 93: 237-48.
- Eliason MJ, Schafer J, Archer B, Capra G (2021) Impact on nasal septal anatomy and physiology following Le Fort I osteotomy. J Craniofac Surg. 32: 277–81.
- Raffaini M, Cocconi R, Spinelli G, Agostini T (2018) Simultaneous rhinoseptoplasty and orthognathic surgery. Aesthetic Plast Surg. 42: 1090-100.
- Seah TE, Ilankovan V (2023) Rhinoplasty as an adjunct to orthognathic surgery. Oral Maxillofac Surg Clin North Am. 35: 115-26.
- Roithmann R (2018) Inferior turbinectomy: what is the best technique? Braz J Otorhinolaryngol. 84: 133-4.
- Abdullah B, Singh S (2021) Surgical interventions for inferior turbinate hypertrophy. Int J Environ Res Public Health. 18: 3441.
- Foraster JB (2021) Nasal dorsum reduction simultaneous to orthognathic surgery. Facial Plast Surg. 37: 646-50.
- Robotti E (2018) Shaping the nasal dorsum. HNO. 66: 92-102.
- Guyuron B, Rune A, Afrooz PN (2008) Correction of nasal base deformities with the alar cinch suture. Aesthet Surg J. 28: 257-64.
- Peled M, Laufer D, Gutman D (1992) Alar base cinch suture following Le Fort I osteotomy: Rationale and technique. Int J Oral Maxillofac Surg. 21: 307-9.
FIGURE 1
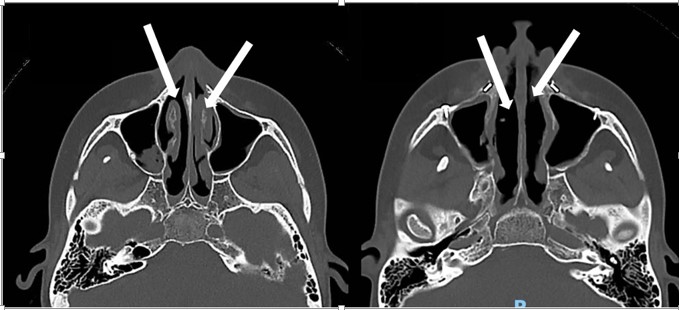
Figure 1: Patient male, 36 yo, underwent orthognathic surgery to improve breathing. The TC show inferior turbinectomy concomitant with orthognathic surgery, increasing nasal airflow. Axial TC. A) Before orthognathic surgery. Hypertrophy inferior turbinates. B) After orthognathic surgery with turbinectomy and the large space into the nose
FIGURE 2
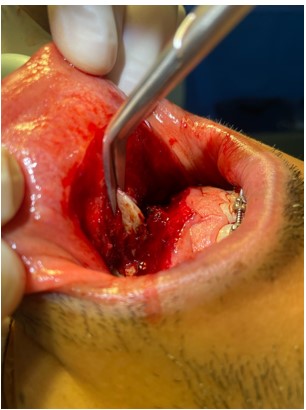
Figure 2: Nasal septum exposure and graft remove
FIGURE 3

Figure 3: Before Orthognathic surgery B) After Orthognathic surgery and septum graft in nasal tip, alar cinch suture and Inferior Turbinate Reduction
Tables at a glance
Figures at a glance