Multicenter Prospective Randomized Controlled Phase II Clinical Study of Sequential or Simultaneous Whole-Brain Radiotherapy for a Limited Number of Brain Metastases from Non-Small Cell Lung Cancer
Received Date: May 09, 2023 Accepted Date: June 09, 2023 Published Date: June 12, 2023
doi: 10.17303/jcrto.2023.11.103
Citation: Lei Yu, Yu He, Wenxia Ren, Daiyuan Ma (2023) Multicenter Prospective Randomized Controlled Phase II Clinical Study of Sequential or Simultaneous Whole-Brain Radiotherapy for a Limited Number of Brain Metastases from Non-Small Cell Lung Cancer. J Cancer Res Therap Oncol 11: 1-14
Abstract
Objective: This study aimed to compare the neurocognitive damage and treatment efficacy of whole-brain radiotherapy (WBRT) with sequential integrated boost (SEB) or simultaneous integrated boost (SIB) in patients with non-small cell lung cancer (NSCLC) brain metastases.
Methods: 69 NSCLC patients with brain metastases were randomly divided into two groups: group A—30 cases who received WBRT(30Gy/10Fx) + SEB (12Gy/3Fx); group B-39 cases who received WBRT(30Gy/10Fx) + SIB (40Gy/10Fx). For all patients, a mini-mental state examination (MMSE) was performed before radiotherapy, at the end of radiotherapy, and 1 to 6 months after radiotherapy, and the differences in neurocognitive function between the two groups were compared. To assess the size of intracranial lesions and compare the objective remission rate (ORR), local control rate (DCR), and 6-- month progression-free survival (PFS) rate of brain metastases in the two groups, enhanced MRI was performed on all patients at 1 and 6 months following radiotherapy.
Results: Both groups showed a statistically significant (P< 0.05) and progressive decrease in MMSE scores after radiotherapy. For group A, the MMSE scores for 1, 3, and 6 months after radiotherapy were 23.21±3.1, 22.65±3.77, and 22.41±3.43. Group B were 22.38±4.62, 21.28±4.35, and 21.19±4.13. There was a statistically significant difference between the MMSE scores of the two groups 1 month after radiotherapy compared with 3 months after radiotherapy (P< 0.05). In the subgroup of patients with ≤3 brain metastasis, the MMSE scores of groups A and B were 23.710±2.998 and 20.890±4.263 in 3 months after radiotherapy, and the difference was statistically significant compared with baseline (P< 0.05). The treatment efficacy was assessed at 1 and 6 months after radiotherapy, and there was no significant difference in the ORR, DCR, and 6-month PFS rates between the two groups
Conclusion: Both WBRT+SEB and WBRT+SIB negatively affect neurocognitive function in NSCLC patients with brain metastases 1 to 6 months after radiotherapy, and the most severe effects were observed 3 months after radiotherapy. In patients with ≤3 brain metastases, WBRT+SEB was less detrimental to neurocognitive function than WBRT+SIB. The treatment efficacy of the two approaches did not significantly differ
Keywords: Brain metastases; Non-small cell lung cancer; Neurocognitive function; Simultaneous boost; Sequential boost; Whole-brain radiotherapy
Introduction
Lung cancer is the deadliest cancer in the world [1], with non-small cell lung cancer (NSCLC) accounting for the majority. NSCLC frequently metastasizes to the central nervous system, with 10% of patients present with brain metastases (BM) at the time of initial diagnosis and >25% of patients having BM during treatment [2]. Patients with BM often have a poor prognosis, and the survival of patients with symptomatic BMs is ~1–3 months if left untreated [3]. Currently, the treatment of BM mainly includes radiotherapy, surgery, chemotherapy, targeted therapy, immunotherapy, and palliative therapy [4]. Since surgery is mainly applicable to patients with a single BM lesion [5], and chemotherapy drugs have limited efficacy due to penetration of the blood-brain barrier [6], radiotherapy remains the primary treatment option for patients with BM. However, the neurocognitive decline caused by radiation brain injury also seriously affects the quality of survival of patients. Whole brain radiotherapy (WBRT) and stereotactic radiosurgery (SRS) are currently the main treatments for unresectable brain metastases (BM). WBRT has a better local control rate but has a detrimental effect on patients’ neurocognitive function [7]. Even though SRS has less impact on neurocognitive function than WBRT, it also has less intracranial tumor control rate [8]. Therefore, combining the two may bring double benefits. At present, there are two primary boost schemes: sequential integrated boost (SEB), in which the boost dose is delivered after WBRT, and simultaneous integrated boost (SIB), in which the boost dose is delivered within a fraction but varied throughout the course the treatment [9-11]. Today, there is a growing concern about the quality of patient survival. A previous study [12] showed that compared with WBRT+SIB, WBRT+SEB showed improved survival for NSCLC patients with BM, especially in cohorts of male patients, patients < 60 years old, and patients with oligometastatic disease. Both treatments led to a marked reduction of neurocognitive function 3 months after radiotherapy compared with baseline. However, this effect was less pronounced in patients receiving WBRT+SEB. The results from this study are limited due to the small sample size and retrospective nature of the study from a single center. To address these limitations, we performed a multicenter, prospective, randomized controlled study to compare neurocognitive function and therapeutic efficacy of WBRT combined with SEB or SIB in NSCLC patients with BM.
Different criteria have been proposed to evaluate BM prognosis. In 1997, Gaspar proposed a recursive partitioning analysis (RPA) to evaluate the prognosis of patients with BM according to the patient's Karnofsky Performance Status (KPS) score, age, primary tumor control or not, and whether there is metastasis outside the central nervous system [13]. Patients are categorized into three grades based on RPA, and the median survival time decreases as the RPA grade increases [13]. In 2004, Lorenzoni et al. [14] proposed a simplified version of the basic score for brain metastases (BS-BM) for BM patients treated with stereotactic radiosurgery (SRS) (Table 1). More recently, Sperduto et al. [5] put forward a more detailed grading prognostic assessment (GPA) index. Patients with GPA>4 have the best prognosis (Table 2).
Methods
Clinical InformationThis retrospective study was approved by the Review Board of the Affiliated Hospital of North Sichuan Medical College (No. 2018ER(R)054). From October 2018 to December 2020, 69 patients with symptomatic NSCLC with BM admitted to the Affiliated Hospital of North Sichuan Medical College, Mianyang Central Hospital, Guangyuan Central Hospital, Suining Central Hospital, Dazhou Central Hospital, and Nanchong Central Hospital were enrolled into the study. Inclusion criteria were as follows: (1) the patient's condition was stable and could complete radiotherapy; (2) no contraindication to radiotherapy and ability and willingness to sign the radiotherapy consent form; (4) < 10 intracranial metastases were confirmed by imaging; (5) age 18–80 years, ECOG score standard 0-2 points/KPS≥70 points, estimated survival time>1 month; (6) the maximum diameter of intracranial lesions≤5cm; (7) extracranial lesions received systematic treatment as planned; (8) ability to cooperate in MMSE scoring
Exclusion criteria were as follows: (1) history of other malignant tumors except for NSCLC BM; (2) pregnancy or lactation; (3) participation in other clinical trials; (4) serious complications, including severe heart rate arrhythmia, severe cerebrovascular disease, and psychosis; (5) no regular follow-up conditions, poor compliance; (6) inability to receive MRI or CT examination; (7) the dose requirement of radiotherapy prescription could not be met.
Treatment planA total of 69 patients were randomly divided into group A (WBRT+SEB) or group B (WBRT+SIB). Before radiotherapy, skull-enhanced CT was used for localization. The target area was delineated after the localization image was fused with the skull-enhanced MRI image through the MIM Software Beijing Co., Ltd. The clinical target volume (CTV) was the whole brain, and the planning target volume (PTV) was defined as a 5 mm margin to the CTV; the gross tumor volume (GTV) was the metastasis, and P-GTV was defined as a 2 mm margin to the GTV. The prescription dose of WBRT in group A was 30Gy/10Fx(5 fractions per week), followed by repositioning; for metastatic focus, the dose was 12Gy/3Fx (Figure1-2). The prescription dose of WBRT in group B was 30Gy/10Fx (5 fractions per week), and the corresponding dose for metastatic focus was 40- Gy/10Fx (Figure 3). All treatments were delivered using intensity-modulated RT (IMRT) by 6MV X-ray medical linear accelerators (Elekta Synergy).
ObservationsWe performed MMSE scoring before radiotherapy, at the end of radiotherapy, and 1, 3, and 6 months after radiotherapy to evaluate patients’ neurocognitive function. In addition, the patients were subjected to brain-enhanced MRI 1 and 6 months after radiotherapy, using WHO standards. CR: complete disappearance of lesions can be seen for at least 1 month; PR: the product of the two paths of tumor decreased by more than 50%, and other lesions did not increase significantly, at least 1 month; SD: tumor two-diameter product shrinkage of less than 50% or enlargement of less than 25%, at least 1 month; PD: one or more lesions with a two-path product increase of more than 25% or new lesions. The overall response rate (ORR) was defined as (PR+CR)/total number of cases×100%. The disease control rate (DCR) was defined as (SD+CR+PR)/total number of cases×100%. The progression-free survival (PFS) rate of intracranial lesions in June was defined as (SD+CR+PR)/total number of cases×100%.
Statistical analysisAll statistical analyses were performed using the SPSS 22.0 software. Normally distributed variables were described as mean and standard deviation. Independent samples were used to test the differences between groups, and paired samples were used to test the differences within groups. Other quantities were compared by either chisquare (χ2 ) or Fisher's exact test. P< 0.05 was considered statistically significant
Results
Patient characteristics and manifestationsA total of 72 eligible cases were initially included in this study. Three patients who discontinued radiotherapy were excluded, and 69 cases were finally included in the study. Tables 3 and 4 summarize the clinical characteristics of the two groups of patients.
Differences between the two groups of patients at each treatment stage
There was no significant difference in MMSE scores between the two groups at each treatment stage (P>0.05) (Table 5).
Changes in the neurocognitive function of patients in group A (WBRT+SEB) at different treatment stages
The MMSE scores at 1, 3, and 6 months after radiotherapy were significantly lower than those before radiotherapy (P< 0.05). There was no significant difference between the MMSE score at the end of radiotherapy and before radiotherapy (P>0.05). There was a significant difference in MMSE scores between 3 months after radiotherapy and 1 month after radiotherapy (P< 0.05). There was no significant difference in MMSE score between 6 months after radiotherapy and 3 months after radiotherapy (P>0.05). It shows that in the SEB group, the most substantial impairment of the neurocognitive function was observed 3 months after radiotherapy and that this impairment improved 6 months after radiotherapy (Table 6).
Changes in the neurocognitive function of patients in group B (WBRT+SIB) at different treatment stages
rence in MMSE scores between 3 and 1 months after radiotherapy (P< 0.05). There was no significant difference in MMSE score between 6 and 3 months after radiotherapy (P> 0.05). It shows that in the SIB group, the neurocognitive function deterioration is the most pronounced at 3 months after radiotherapy and alleviates 6 months after radiotherapy (Table 7).
Changes of neurocognitive function in different treatment stages of two treatment methods in each subgroup
We found that age, gender, EGFR/ALK/ROS1 driver gene mutation, pathological type of breast cancer, and KPS score had no effect on MMSE scores between the two methods at each treatment stage (P>0.05) (Tables 8, 9, 10,11,12).
There was no significant difference in MMSE scores among patients with ≥3 intracranial metastases at each treatment stage (P>0.05); in patients with ≤3 intracranial metastases, there was a statistically significant difference in MMSE scores at the end of radiotherapy and 3 months after radiotherapy (P< 0.05) (Table 13). These data suggest that in patients with ≤3 intracranial metastases, the neurocognitive damage caused by the SEB regimen at the end of radiotherapy and 3 months after radiotherapy was lower than that caused by the SIB regimen.
DCR and ORRThe DCR of group A was 96.00%, while that of group B was 94.30%, with no significant difference between groups (P>0.05) (Table 14). The ORRs of groups A and B were 84.00% and 80.00%, respectively, also without significant difference (P>0.05) (Table 14). These findings indicate no difference in DCR and ORR between the two treatment regimens.
6-month PFSThe 6-month PFS rates of intracranial metastases in the two groups were 50.0% and 58.6%, respectively (P>0.05). These data indicate no significant difference between the two regimens regarding treatment efficiency. (Table 15).
Discussion
In this study, 69 patients with NSCLC BM were analyzed to compare the advantages and disadvantages of WBRT+SEB and WBRT+SIB. Our primary goal was to evaluate the effect of these therapeutic regimens on cognitive function and BM survival. Compared with baseline, the MMSE score was significantly reduced in both groups at 1, 3, and 6 months after radiotherapy (P< 0.05), indicating that the neurocognitive function decreased in both groups during 6 months’ post-radiotherapy. However, the decline rate of the WBRT+SEB group was much less pronounced. In patients with ≤3 intracranial metastases, we observed that the WBRT+SIB group had a significantly lower MMSE score than the WBRT+SEB group (P< 0.05), indicating that the SEB regimen inflicted less damage to the neurocognitive function 3 months after radiotherapy. We observed no statistically significant difference in MMSE scores between 6 and 3 months after radiotherapy. Therefore, we believe that in patients with neurocognitive impairment, it is most pronounced 3 months after radiotherapy and may recover in 1 year or more after radiotherapy. Finally, there was no difference between ORR, DCR, and 6-month PFS rates between the groups, suggesting that BM progression is not particularly vulnerable to sequential or concurrent radiotherapy regimens.
Our results are consistent with previously published research. Luo et al. [15] found no significant difference in the treatment effect, adverse reactions, and survival rate between WBRT+SEB and WBRT+SIB groups across 80 patients with NSCLC BM. However, Li [16] demonstrated better survival and treatment efficacy for the WBRT+SIB regimen compared with the WBRT+SEB treatment in 65 patients with NSCLC BM. There was no statistical difference between the two treatment methods in the incidence of acute and late radiation injury.
WBRT is closely related to neurocognitive function impairment because radiation damage to the hippocampus is associated with declining learning ability and memory [17.18]. Therefore, when BM patients are treated with WBRT, targeting the hippocampus should be avoided to protect cognitive function. With the progress of radiotherapy technology, implementing hippocampal protective WBRT is feasible. In this study, the patients were not treated with hippocampal protective WBRT, which may have a certain impact on the assessment of neurocognitive impairment.
This study has several limitations, including a short observation time and a small sample size. Moreover, there may be a small discrepancy in MMSE scoring among participating centers. This study did not use hippocampal protection. We plan to employ hippocampal protective WBRT in future studies to further compare the advantages and disadvantages of the two treatment methods
In conclusion, both WBRT+SEB and WBRT+SIB treatment regimens negatively affected neurocognitive function in NSCLC patients with BM. In patients with ≤3 BMs, WBRT+SEB had less effect on neurocognitive function than WBRT+SIB. There was no difference in treatment efficacy between the two approaches. More research is needed to identify the optimal radiotherapy treatment regimen for patients with BM.
- Sung H, Ferlay J, Siegel RL et al. (2021) Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 71: 209-49.
- Langer CJ, Mehta MP (2005) Current management of brain metastases, with a focus on systemic options[J]. Clin Oncol 23: 6207-19.
- Scoccianti S, Ricardi U (2012) Treatment of brain metastases: review of phase III randomized controlled trials[J]. Radiotherapy and oncology: journal of the European Society for Therapeutic Radiology and Oncology 102: 168-79.
- Lorenzoni J, Devriendt D, Massager N et al. (2004) Radiosurgery for treatment of brain metastases: estimation of patient eligibility using three stratification systems[J]. Int J Radiat Oncol Biol Phys 60: 218-24.
- Ammannagari N, Ahmed S, Patel A et al. (2013) Radiological response of brain metastases to novel tyrosine kinase inhibitor lapatinib[J]. QJM Monthly Journal of the Association of Physicians 106: 869-70.
- Weidle UH, Niewöhner J, Tiefenthaler G (2015) The Blood-Brain Barrier Challenge for the Treatment of Brain Cancer, Secondary Brain Metastases, and Neurological Diseases[J]. Cancer Genomics Proteomics 12: 167-77.
- Weidle UH, Niewöhner J, Tiefenthaler G (2015) The Blood-Brain Barrier Challenge for the Treatment of Brain Cancer, Secondary Brain Metastases, and Neurological Diseases[J]. Cancer Genomics Proteomics 12: 167-77.
- Madden DJ, Spaniol J, Costello MC et al. (2009) Cerebral white matter integrity mediates adult age differences in cognitiveperformance[J]. Journal of cognitive neuroscience 21: 289-302.
- Brown PD, Jaeckle K, Ballman KV et al. (2016) Effect of Radiosurgery Alone vs Radiosurgery With Whole Brain Radiation Therapy on Cognitive Function in Patients With 1 to 3 Brain Metastases: A Randomized Clinical Trial[J]. JAMA 316: 401-9.
- Rodrigues G, Yartsev S, Yaremko B et al. (2011) Phase I trial of simultaneous in-field boost with helical tomotherapy for patients with one to three brain metastases. Int J Radiat Oncol Biol Phys 80: 1128-33.
- Rodrigues G, Yartsev S, Tay KY, Pond GR, Lagerwaard F, Bauman G (2012) A phase II multi-institutional study assessing simultaneous infield boost helical tomotherapy for 1–3 brain metastases. Radiat Oncol 7: 42.
- Rodrigues G, Eppinga W, Lagerwaard F et al. (2012) A pooled analysis of arc-based image-guided simultaneous integrated boost radiation therapy for oligometastatic brain metastases. Radiother Oncol 102: 180-6.
- Qing D, Zhao B, Zhou YC et al. (2020) Whole-brain radiotherapy plus sequential or simultaneous integrated boost for the treatment of a limited number of brain metastases in non-small cell lung cancer: A single-institution study[J]. Cancer Med 9: 238-46.
- Laurie E, Gaspar et al. (2000) Validation of the RTOG recursive partitioning analysis (RPA) classification for brain metastases - ScienceDirect[J]. International Journal of Radiation Oncology Biology Physics 47: 1001-6.
- Lorenzoni J, Devriendt D, Massager N et al. (2004) Radiosurgery for treatment of brain metastases: estimation of patient eligibility using three stratification systems[J]. Int J Radiat Oncol Biol Phys 60: 218-24.
- Luo Qingbin, Liu Tiebin, Qi Sheng et al. (2020) To evaluate the efficacy of sequential dose and concurrent dose after whole brain radiotherapy in patients with brain metastases from non-small cell lung cancer [J]. Chinese Medical Guide 18: 81-2.
- Li Jinzhuan (2016) Comparison of NSCLC efficacy between simultaneous push conformal radiotherapy and whole brain radiotherapy with sequential push conformal radiotherapy for 1-3 brain metastases [D]. Guangxi Medical University.
- Lee G, Besse L, Lamba N et al. (2021) Feasibility of hippocampal avoidance whole brain radiation in patients with hippocampal involvement: Data from a prospective study[J]. Med Dosim 46: 21-8.
- Kazda T, Vrzal M, Prochazka T et al. (2017) Left hippocampus sparing whole brain radiotherapy (WBRT): A planning study[J]. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 161: 397-402.
FIGURE 1
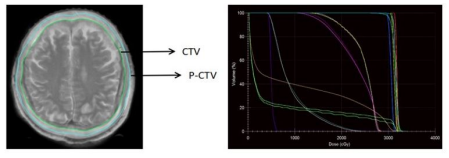
Figure 1: Target area map (left) and DVH diagram of group A at the first stage
FIGURE 2
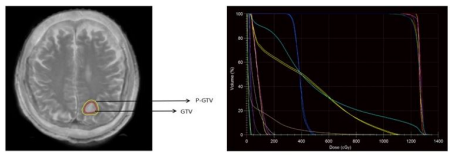
Figure 2: Target area diagram (left) and DVH diagram (diagram) of group A at the first stage
FIGURE 3
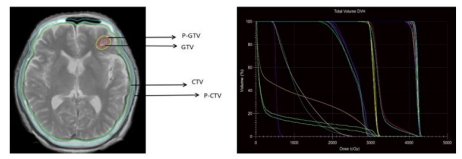
Supplementary Figure 1: Target area map (left) and DVH diagram (right) of group B
Tables at a glance
Figures at a glance