Unilateral Panopthalmitis In Dengue Fever A Rare and Preventable Complication
Received Date: May 05, 2020 Accepted Date: May 17, 2020 Published Date: May 20, 2020
doi: 10.17303/jooa.2020.4.101
Citation:Mayuri Yeole (2020)Unilateral Panopthalmitis In Dengue Fever A Rare and Preventable Complication.J Ophthalmol Open Access 1: 1-4.
Abstract
Objectives: ADengue, one of the most common mosquito borne flavivirus diseases affecting humans, is spread by the Aedes aegypti mosquito. Most people infected with dengue virus are asymptomatic, while in a small proportion it is life-threaten-ing such as Dengue hemorrhagic fever and Dengue shock syndrome. Severe dengue is defined as that associated with severe bleeding, severe organ dysfunction, or severe plasma leakage. One of the complications in Dengue disease that is being ob-served more frequently in recent times is the ophthalmic manifestations. Ophthalmic manifestations can involve both the anterior and posterior segment. However, only a few isolated case reports have been published. Here we report an isolated case of dengue Panopthalmitis, leading to rapidly progressive painful visual loss.
Keywords: Dengue, flavivirus, Aedes aegypti, Panopthalmitis, Severe Dengue
Abbreviations: cfDNA, cell-free DNA; EGFR, epidermal growth factor receptor; NSCLC, non-small cell lung cancer; OS, overall survival; PD, disease progression; PFS, progression-free survival; TKI, tyrosine kinase inhibitor
Introduction
Dengue fever is the most prevalent form of flavivirus infection in humans. The highest incidence occurs in Southeast Asia, India and the American tropics [1,2]. Worldwide cases of illness exceed 100 million per year [2]. Dengue fever is a mosquito borne disease that is commonly found in the tropics. Dengue virus belongs to the Flavivirus genus of the family Flaviviridae and its members include the four antigenically-related serotypes of dengue virus (DENV 1-4). It is transmitted to humans by the bite of an infected female Aedes mosquito, usually the Aedes aegypti mosquito. Dengue hemorrhagic fever (DHF) is a severe and potentially fatal form of the disease. Twenty five thousand deaths are reported annually to the World Health Organization (WHO).
Ophthalmic complications associated with DF and DHF have not been classically described. This complication is being observed more frequently in recent times. However, only a few isolated case reports have been published. Dengue related ocular complications range from 10% to 40% [3,4]. The ocular manifestations range from sub-conjunctival hemorrhage to posterior segment manifestations [5]. The ocular manifestations reported to be associated with dengue infections are mostly posterior segment manifestations like macular edema, vascular occlusions, chorioretinitis, vasculitis with retinal bleeding or cotton wool spots [6,7]. Anterior segment commonly manifests with subconjunctival hemorrhage due to thrombocytopenia [8]. Here we report an unusual manifestation of dengue fever presenting unilaterally with extensive Panopthalmitis.
Case report
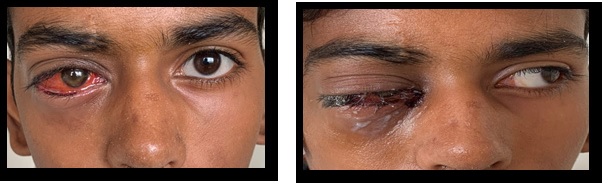
A 14 year old boy presented to us with history of high grade fever since 1 week, associated vomiting since 3-4 days. He had presented with Dengue shock syndrome at other hospital as per history provided, with Dengue NS1 being positive, Platelet count being 33,000/cumm. He was treated for shock as per protocol and transfused with random donor platelets. On day 2 of admission child complained of retro orbital pain, periorbital swelling over the right eye. Patient was brought to us with blood and serous discharge from right eye for further intervention. All hematological investigations were within normal limit, platelet count being 67,000/cumm and Dengue IgM being positive. During the course of treatment we sent culture swab from affected eye, which were negative for any organism. MRI Brain with Orbit was suggestive of right eye proptosis with features of Panopthalmitis, orbital cellulitits and abscess of right eye. On bedside examination, there was no perception to light noted in right eye; whereas the left eye was normal. We started the child on broad spectrum intravenous and topical antibiotics, also systemic steroids on day 2 of admission and saw a significant improvement in restoration of eye movements in right eye except for abduction. He also received periocular antibiotics. Proptosis had eventually reduced with no perception to light, corneal infiltrates present, and fundus was still not visible. He recovered from systemic dengue illness with platelet count at the time of discharge being 1.8 lakh/cumm but still had no perception of light in right eye and was advised for the evisceration, however due to financial constraints patient failed to follow up (figure 1).
Discussion
Dengue is one of the most important emerging viral diseases of humans in India, afflicting humanity in terms of morbidity and mortality [9]. The ocular manifestations of dengue have been reported in all age groups, but more commonly in early thirties [3,6] Vision threatening complications of dengue have been reported at the end of 1st week of dengue fever as this is the phase coinciding with nadir of thrombocytopenia [6]. Panopthalmitis is a rare complication, which has been reported in only 2 cases in literature till date [10,11].
Panopthalmitis is a severe involvement of the anterior and the posterior segments of the eye, presenting with marked lid edema, proptosis, limitation of ocular movements and high IOP. The common symptoms include ocular pain, blurring of vision, and ocular discharge. During the later stages of infection, the patients may develop severe inflammation with chemosis, proptosis, and hypopyon that can lead to blindness [12]. Though the pathogenesis of these changes is not yet known, their clinical presentation and behavior are indicative of an immunogenic etiology rather than infective [13]. The course of the ocular complications, such as systemic DF, is generally self-limiting. However, immediate high dose steroids at presentation, followed by a rapid taper, has been suggested and tried with varying success to suppress and minimize the inflammatory damage [14].
Proptosis in dengue fever could be due to retro bulbar hemorrhage or panophthalmitis [10]. Possible mechanism for globe rupture could be an increase in intraocular and intraorbital pressure secondary to retro bulbar, suprachoroidal, and intravitreal hemorrhages [15,16]. Exact etiology of Panopthalmitis is not known. It may be due to the viremia causing embolization of infective material through retinal vessels, occurring at the nadir in platelet count. After establishing a septic focus in the retina, infection could have disseminated throughout the retina, vitreous, and anterior segment [11].
Panopthalmitis, though rare in dengue, is vision-threatening. Hence, a systematic ophthalmic examination and intervention in dengue patients with ocular symptoms is mandatory. Physicians should be aware and vigilant toward patients with dengue related ophthalmic complaints, as the patients may develop life threatening Panopthalmitis.
Conclusion
The onset of visual symptoms usually occurs at the lowest platelet level, blurring of vision typically coincides with the nadir of thrombocytopenia and occurs close to one week after onset of fever. Hence a very careful observation by fundus examination may be required during this period. The clinical features of dengue retinopathy includes any one or all of the following such as retinal edema, blot hemorrhages, cotton wool spots, anterior uveitis, exudative retinal detachment [12]. Even though the disease is self-limiting and has a good prognosis it can also result in Panopthalmitis and vision loss. Topical, periocular, oral, intravenous antibiotics, steroids and immunoglobulins have been advocated for the management of dengue associated uveitis and optic neuritis. The inference is that the clinicians should have heightened awareness of dengue related ophthalmic complications and should facilitate prompt referral for ophthalmic assessment and management, with early administration of steroids systemic or intraviterous might help in halting the ocular damage.
- Halstead SB (1966) Mosquito-borne hemorrhagic fevers of South and South-east Asia. Bull World Health Organ. 35:3.
- Halstead SB (1990) Global epidemiology of dengue hemorrhagic fever. Southeast Asian J Trop Med Public Health.21:636
- Kapoor HK, Bhai S, John M, Xavier J (2006) Ocular manifestations of dengue fever in an East Indian epidemic. Can J Ophthalmol. 41:741-46
- Su DH, Bacsal K, Chee SP, Flores JV, Lim WK, Cheng BC et al. (2007) Dengue Maculopathy Study Group. Prevalence of dengue maculopathy in patients hospitalized for dengue fever. Ophthalmology 114:1743-47
- Ranjan S, Ranjan R (2013) Dengue-related Ocular Pathology: A review. International Journal of Biomedical Research 4:451-60
- Chan DP, Teoh SC, Tan CS, Nah GK, Rajgopalan R, Prabhakar Gupta MK et al. (2006) The Eye Institute Dengue- Related Ophthalmic Complications Workgroup: Ophthalmic complications of dengue. Emerg Infect Dis 12: 285-89
- Lim WK, Mathur R, Koh A, Yeoh R, Chee SP (2004) Ocular manifestations of dengue fever. Ophthalmology. 111: 2057–64
- Wen KH, Sheu MM, Chung CB, Wang HZ, Chen CW (1989) The ocular fundus findings in dengue fever. The Kaohsiung Journal of Medical Sciences 5:24-30.
- Saranappa SB, Sowbhagya HN (2012) Panophthalmitis in dengue fever. Indian Pediatr 49:760.
- Sriram S, Kavalakatt JA, Pereira AD, Murty S (2015) Bilateral panophthalmitis in dengue fever. Ann Trop Med Public Health 8:217-8.
- Okada AA, Johnson RP, Liles WC, D’Amico DJ, Baker AS (1994) Endogenous bacterial endophthalmitis. Report of a 10-year retrospective study. Ophthalmology 101:832-8.
- Teoh SC, Chan DP, Nah GK, Rajagopalan R, Laude A, Ang BS, et al. (2006) A Re-look at Ocular Complications in Dengue Fever and DHF. Dengue Bull. 30
- Teoh SC, Chan DP, Augustinus L, Chee CK, Lim TH, Goh KY (2006) The Eye Institute Dengue Related Ophthalmic Complications Workgroup. Dengue chorioretinitis and denguerelated ophthalmic complications. Emerg Infect Dis 12:285-9
- Nagaraj KB, Jayadev C, Yajmaan S, Prakash S (2014) An unusual ocular emergency in severe dengue. Middle East Afr J Ophthalmol 21:347-9.
- Kulkarni AG, Athale N, Sheth K, Rathi A, Shinde V, Deshmukh S, et al. (2016) Globe rupture – A rare ocular manifestation of dengue fever in convalescent phase. Int J Sci Res 5:1727-9.
FIGURE 1
Figure 1: Pre and post systemic steroid response
FIGURE 2

Figure 2: Photograph of the compact glass cell #2 especially designed for this study.
FIGURE 3

Figure 3: Block diagram of the experimental setup
FIGURE 4

Figure 4: Resonance frequency, Q-factor and cell #1 response in function of the mesh quality (�1� = Extremely fine and �9� = Extremely coarse)
FIGURE 5

Figure 5: Microphones A and B responses for cell #1 in the function of the excitation frequency. Experimental data are represented by dots whereas modeling results are in solid line.
FIGURE 6

Figure 6: Cell #1 response in function of the excitation frequency. Experimental data are represented by dots whereas modeling results are in solid line.
FIGURE 7

Figure 7: Resonance frequency, Q-factor and cell #2 response in function of the mesh quality (�1� = Extremely fine and �9� = Extremely coarse)
FIGURE 8

Figure 8: Microphones A and B responses for cell #2 in function of the excitation frequency. Experimental data are represented by dots whereas modeling results are in dashed line for PAM, in solid line for TAM-BL and in dotted line for TAM-BL with model including leaks.
FIGURE 9

Figure 9: Cell #2 response in function of the excitation frequency. Experimental data are represented by dots whereas modeling results are in dashed line for PAM, in solid line for TAM-BL and in dotted line for TAM-BL with a model including leaks.
Figures at a glance