Endoscopic Retrograde Cholangiopancreatography in Hepatic Hydatid Disease
Received Date:September 09, 2020 Accepted Date:September 25, 2020 Published Date: September 30, 2020
doi: 10.17303/ejmrc.2020.2.101
Citation:H. Hassine (2020) Endoscopic Retrograde Cholangiopancreatography in Hepatic Hydatid Disease. Eur J Med Res Clin Trials 1: 1-3
Abstract
Hydatid disease (HD) is a parasitic infection commonly caused by the larva of Echinococcus granulosus mostly located in the liver. Complicated HD is frequent. While surgical treatment was the traditional first choice, endoscopic retrograde cholangiopancreatography (ERCP) has become the treatment of choice for the management of complicated forms. ERCP is a safe and effective way to manage biliary pre and post-operative complications of Hepatic HD.
Keywords:Hydatid disease; Liver; ERCP
Introduction
Hydatid disease (HD) is a parasitic infection commonly caused by the larva of Echinococcus granulosus, mostly seen in North Africa, the Middle East, and South America [1, 2]. HD remains a serious medical health problem. The liver is the most frequently involved site (50 – 70% of patients) followed by the lungs (15%). Intrabiliary rupture of a hepatic hydatid cyst with subsequent fistula formation is a common complication reported in 5 – 25% of cases [3]. Biliary leakage is the most frequent postoperative complication following surgery for hydatid cysts of the liver. While surgical treatment was the traditional choice, endoscopic retrograde cholangiopancreatography has become the treatment of choice for the management of intrabiliary hydatid rupture and other postoperative complications [4].
Methods
The bibliographic search was conducted using the following sites: Cochrane and Pubmed. The keywords used were: hydatid disease, Echinococcus granulosus, ERCP.
Clinical Presentation
Slow larval growth results in an asymptomatic phase for a long period of time. Presenting symptoms depend on the number, size of cysts, and the presence of complications [5, 6]. Symptoms also depend on the mass effect within the liver and upon surrounding structures and organs [5]. Non-complicated hydatid cysts of the liver are asymptomatic or may present with hepatomegaly, jaundice, and right or epigastric pain. Nonspecific symptoms such as nausea, vomiting, and fever may also be present [6]. Intrabiliary rupture, direct rupture into the abdominal cavity, and hydatid cyst superinfection is the most frequently encountered complications [7]. Cyst rupture may be responsible for anaphylaxis reaction [5]. The clinical presentation of intrabiliary rupture can range from asymptomatic to jaundice, cholangitis, liver abscess, pancreatitis, cholecystitis, or septicemia depending on the size of the cystobiliary communication. Post-operative complications are biliary benign strictures; post-surgical external biliary fistula; residual intrabiliary debris and secondary sclerosing cholangitis.
Endoscopic retrograde cholangiopancreatography in management of complicated hepatic hydatid disease
Surgical management of biliary fistulas is associated with high morbidity and mortality [4]. Endoscopic retrograde cholangiopancreatography (ERCP) is now the mainstay treatment modality for pre and postoperative biliary complications of hepatic HD [8].
Endoscopic sphincterotomy (ES) reduces the pressure gradient between the bile duct and the duodenum. This technique allows diverting bile away from the site of the leak leading to fistula healing. Prior to surgery, ERCP was found to be beneficial in patients with acute cholangitis, internal fistulae, and daughter vesicles in the bile ducts and sphincterotomy led to successful internal drainage. ES is reported to help in preventing postoperative complications such as external biliary fistulae [9].
ERCP is also very beneficial in patients with early postoperative complications such as persistent biliary fistula and obstructive jaundice due to hydatid cyst surgery whereas secondary sclerosing cholangitis and stenosis of the sphincter of Oddi are considered as late postoperative complications [10, 11]. ES alone may be sufficient to heal postoperative external biliary fistula [9].
In Tunisians patients who had undergone previous surgery, the indications of the ERCP were persistent external biliary fistulae (77%), overcome obstruction or cholangitis due to residual materials within bile duct (21%), and secondary biliary stricture (2%). ES was then performed in all cases with satisfactory results. Two patients required biliary stenting due to stricture of the bile duct and two others required nasobiliary drainage [12].
The nasobiliary drain or stent bridges the defect at the site of the leak, providing a conduit for bile flow [4].
Conclusion
ERCP is a safe and effective way to manage biliary pre and post operative complications of Hepatic HD. In most patients, ES is the most efficient treatment of intrabiliary cyst rupture, postoperative external biliary fistulas, jaundice and accompanying cholangitis. In some cases, biliary stenting or nasobiliary drainage may be required.
- MC manus Dp, zhang w, Li J, bartley Pb (2003) Echinococcosis. Lancet 362: 1295-1304.
- Eckert j, deplazes p (2004) Biological, epidemiological, and clinical aspects of echinococcosis, a zoonosis of increasing concern. Clin Microbiol Rev. 17: 107-135.
- Erzurumlu K, dervisoglu A, polat C, senyurek G, yetim I, hokelek M (2005) Intrabiliary rupture: an algorithm in the treatment of controversial complication of hepatic hydatidosis. World J Gastroenterol 11: 2472-2476.
- Sharma BC, Reddy RS, Garg V (2011) Endoscopic management of hepatic hydatid cyst with biliary communication. Digestive Endoscopy 24: 267–270.
- Nunnari g, pinzone MR, gruttadauria S, celesia BM, madeddu G, malaguarnera G, et al. (2012) Hepatic echinococcosis: clinical and therapeutic aspects. World J Gastroenterol 18: 1448-1458.
- Sayek I, onat D (2001) Diagnosis and treatment of uncomplicated hydatid cyst of the liver. World J Surg. 25: 21-27.
- Alghofaily KA, Saeedan MB, Aljohani IM, Alrasheed M, Mcwilliams S, Aldosary A, et al. (2017) Hepatic hydatid disease complications: a review of imaging findings and clinical implications. Abdominal Radiol. 42: 199-210.
- Ozturk G, Polat KY, Yildirgan MI, Aydinli B, Atamanalp SS, et al. (2009) Endoscopic retrograde cholangiopancreatography in hepatic alveolar echinococcosis. J Gastroentero Hepatol. 24: 1365–1369.
- Dumas R, Le gall P, Hastier P, Buckley MJM, Conio M, Delmont JP (1999) The Role of endoscopic retrograde cholangiopancreatography in the management of hepatic hydatid disease. Endoscopy. 31: 242–247.
- Agarwal S, Sikora SS, Kumar A, Saxena R, Kapoor VK (2005) Bile leaks following surgery for hepatic hydatid disease. Indian J Gastroenterol 24: 55–58.
- Dolay k, Akbulut S (2014) Role of endoscopic retrograde cholangiopancreatography in the management of hepatic hydatid disease. World J Gastroenterol. 20: 15253–15261.
- Hassine h, Sabbah M, Bibani N, Trad D, Elloumi H, Gargouri D, et al. (2017) Place of endoscopic retrograde cholangiopancreatography (ERCP) in the management of hepatic hydatid disease. United European Gastroenterol J. 5 (Suppl 1).
FIGURE 1
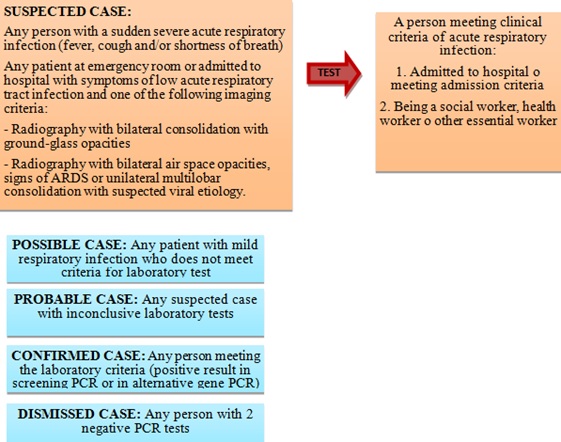
Figure 1: Diagnosis of COVID-19 and clinical classification.
FIGURE 2
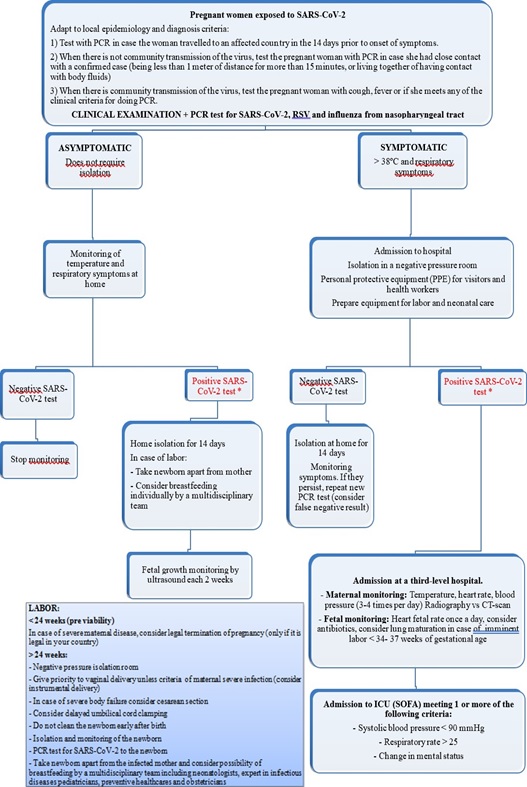
Figure 2: Algorithm of managing pregnant women with suspicion of SARS-CoV-2
FIGURE 3
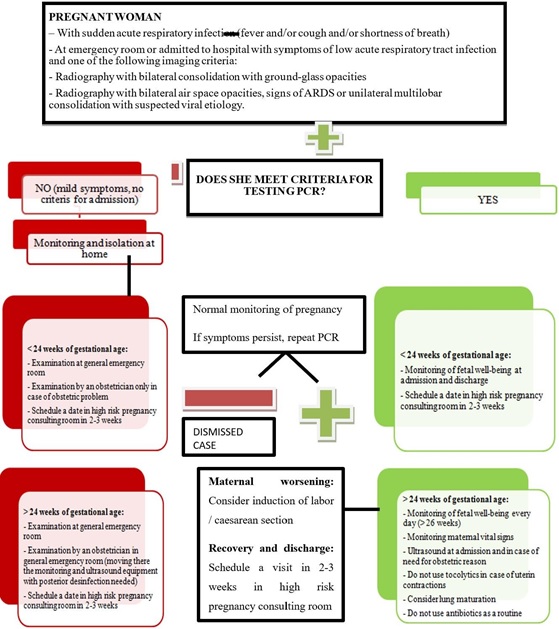
Figure 3:Algorithm of managing pregnant women with suspicion of COVID-19. Adaptation to our institution
Tables at a glance